


EDITORIAL
The article is devoted to the key research directions presented in the third issue of the journal for 2026. The materials of this issue reflect the transition of contemporary science from traditional clinical observation and pathogenetic analysis to digital prediction, personalized risk assessment, and interdisciplinary interpretation of data. Particular attention is paid to publications addressing the use of artificial intelligence and machine learning for predicting pregnancy complications, as well as the need for critical assessment of source data quality, external validation, and clinical applicability of such models. In addition, the article discusses studies focused on hemostatic disorders, endothelial dysfunction, preeclampsia, reproductive health, gynecologic oncology, assisted reproductive technologies, and cancer-associated thrombosis. In the context of the growing role of digital technologies and generative artificial intelligence in medical science, the importance of methodological rigor, scientific continuity, and authorial responsibility is emphasized. The editorial board is concerned about the increasing number of manuscripts submitted by paper mills.
ОRIGINAL ARTICLES
What is already known about this subject?
► Cerebrovascular disorders in pregnant women are associated with hypercoagulable states that develop under the influence of both physiological gestational changes and latent thrombophilic factors, including antiphospholipid antibodies (aPLs) and metabolic disturbances.
► Thrombophilia, both inherited and acquired, is regarded as a significant risk factor for arterial and venous thrombosis as well as for adverse pregnancy outcomes in reproductive age women
► Current approaches to prevent thrombotic complications in pregnant women include the use of anticoagulants and antiplatelet agents; however, questions regarding the optimal timing for treatment initiation and the risk stratification criteria in patients with cerebrovascular pathology remain.
What are the new findings?
► Latent thrombophilic conditions are frequently detected in pregnant and reproductive-age women with an adverse cerebrovascular history, as well as in patients at high risk of acute cerebrovascular events (ACVEs) identified by using a previously developed prognostic model, and often have a combined pattern.
► It was shown that the pattern of latent thrombophilic conditions in this category of patients includes not only genetic forms of thrombophilia, but also aPLs, hyperhomocysteinemia, and altered vWF/ADAMTS-13 axis.
► The data obtained confirm the multifactorial nature of prothrombotic predisposition in patients with an adverse cerebrovascular history and ACVEs high risk.
How might it impact on clinical practice in the foreseeable future?
► The findings underscore the clinical significance of extended clinical and hemostasiological assessment in pregnant and reproductive-age women with an adverse cerebrovascular history, as well as in patients at high ACVEs risk.
► A comprehensive evaluation of genetic and acquired disorders of the hemostatic system may contribute to more accurate risk stratification and a more evidence-based selection of patients for preventive interventions.
► Early initiation of prophylactic therapy may be considered a clinically justified management strategy for patients with thrombophilia and a history of cerebrovascular disorders.
Aim: to assess the prevalence and pattern of latent thrombophilic conditions in pregnant and reproductive-age women with an adverse cerebrovascular history, as well as in patients at high risk of acute cerebrovascular events (ACVEs) identified using a previously developed prognostic model, based on a comprehensive clinical and hemostasiological analysis.
Materials and Methods. A two-stage observational study was conducted, consisting of sequential retrospective and prospective phases. In the retrospective phase, data from 50 patients with ACVEs that had occurred during pregnancy, in the early postpartum period, or outside gestation were analyzed; 30 clinically healthy pregnant women were included in control group. Based on the retrospective data, a prognostic model for cerebrovascular risk stratification had previously been developed; in the present study, this model was used solely as a tool to identify high-risk patients. In the prospective phase, 45 pregnant and reproductive-age women with ACVEs history or a high risk of their development, as identified by the above model, as well as 30 clinically healthy pregnant women, were examined. All patients underwent an extended clinical and hemostasiological evaluation, including assessing genetic thrombophilia, natural anticoagulant deficiencies, antiphospholipid antibodies (aPL), homocysteine levels, metalloproteinase ADAMTS-13 activity, anti-ADAMTS-13 antibodies, as well as parameters of the vWF/ADAMTS-13 axis.
Results. In the retrospective phase, inherited and acquired forms of thrombophilia were detected significantly more often in patients with ACVEs than in control group, 84.0 % versus 6.7 % cases, respectively. Pattern of cerebrovascular events was featured with ischemic stroke diagnosed in 58.0 % patients, whereas cerebral venous thrombosis – in 42.0 % cases. In prospective group, genetically determined thrombogenic abnormalities were detected in 35.6 % patients, criterial aPLs were detected in 28.9 %, hyperhomocysteinemia – in 15.6 %, reduced ADAMTS-13 activity – in 11.1 %, anti-ADAMTS-13 antibodies – in 26.7 %, and elevated von Willebrand factor levels – in 28.9 %. Combined thrombophilia was identified in 35.6 % patients in the prospective group, suggesting the multifactorial nature of prothrombotic predisposition.
Conclusion. Latent thrombophilic conditions are frequently detected in pregnant and reproductive-age women with ACVEs history, as well as in patients at ACVE high risk, and often have a combined pattern involving both genetically determined and acquired hemostatic disorders. These findings substantiate a need for extended clinical and hemostasiological assessment in this category of patients at the stage of pregnancy planning and during pregnancy to improve risk stratification and individualize prevention of thrombotic complications.
What is already known about this subject?
► Alterations in utero-fetal blood flow account for obstetric and perinatal complications.
► An important role in developing pregnancy pathology is assigned to endothelial status, which determines formation of the fetoplacental system from early pregnancy stage.
► Diagnosis of endothelial dysfunction in pregnant women is of crucial importance in preventing gestational complications.
What are the new findings?
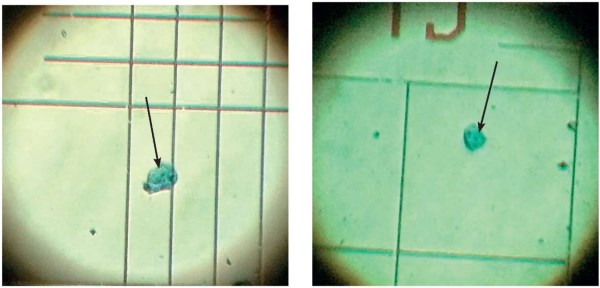
► A method for detecting endothelial dysfunction in pregnant women using morphometric examination of desquamated endothelial cells (DECs) has been developed.
► The study of endothelial dysfunction at the cellular level allows to optimize early diagnosis of vascular disorders in pregnant women.
How might it impact on clinical practice in the foreseeable future?
► DECs morphometry is a minimally invasive, quick-to-perform, economically and technically accessible method of endothelial examination.
► The developed method can be used as an early prenatal diagnostic tool suitable for mass screening in pregnant women for preventing obstetric and perinatal complications.
Aim: improving diagnosis of vascular disorders during pregnancy by using morphometric examination of desquamated endothelial cells (DECs).
Materials and Methods. An observational prospective study assessing endothelial status in pregnant women and fetuses was carried out using the "case-control" method. 180 women in first trimester who had terminated pregnancy were examined: 90 patients were diagnosed with undeveloped pregnancy and instrumental removal of the fetal egg was performed, 90 women had a medical abortion on request. Endothelial dysfunction was diagnosed in all pregnant women, and morphometry of circulating DECs was performed. The data obtained further underwent statistical analysis.
Results. A comparative analysis of endothelial lesion markers in pregnant women demonstrated the diagnostic significance of DECs morphometric examination.
Conclusion. Morphometric examination of peripheral blood DECs may be a diagnostic marker of vascular disorders in pregnant women and represents a promising area to prevent obstetric and perinatal pathology.
What is already known about this subject?
► Vulvovaginal atrophy (VVA), or genitourinary menopausal syn-
drome (GUMS), is associated with estrogen deficiency, which causes epithelial thinning, reduced blood circulation, loss of tissue elasticity, and changed vaginal microbiota composition.
► In postmenopause, a decreased estrogen receptors (ERα) expression in the vaginal epithelium is observed, which is related to histological signs of atrophic changes.
► The serum estradiol level weakly correlates with the severity of symptoms, which indicates the lack of a single objective criterion that comprehensively mirrors receptor apparatus state, epithelium functional activity, and the microbiota.
What are the new findings?
► Epitheliocyte nucleus electrokinetic activity (ENEA) is a sensitive and non-invasive biophysical marker that is closely related to vaginal microbiota state: it decreases proportionately to the degree of dysbiotic disorders.
► ENEA can be used as an additional objective indicator to comprehensively assess the vaginal ecosystem.
► In patients with severe VVA symptoms, there is a decompensation of regulatory processes with a loss of physiological crosstalk, suggesting a potential irreversible cellular changes. In patients with "silent atrophy", due to tissue adaptation and sufficient ERα expression, there is a temporary compensation based on local mechanisms. In women without symptoms, there is a preservation of regulatory crosstalk and the formation of a mechanism for successful adaptation to estrogen deficiency due to preserved receptor arm in epithelial cells.
How might it impact on clinical practice in the foreseeable future?
► For the first time, the biophysical parameter ENEA is proposed to be used as an arm between molecular (receptor) disorders and the clinical as well as VVA microbiological manifestations.
► The data obtained may lay a foundation for creating a novel more precise classification system for patients with VVA, developing criteria for early diagnosis of preclinical stages, and justifying a differentiated approach to treatment based on the state of regulatory crosstalk at the tissue level.
Introduction. Genitourinary menopause syndrome (GUSM) significantly worsens the quality of life of postmenopausal women. Traditional diagnostic approaches based primarily on clinical manifestations provide no precisely assessed severity of pathomorphological disorders.
Aim: to study a relationship between estradiol level, estrogen receptors (ERα) state, the functional activity of vaginal epithelial cells, as well as the characteristics of the vaginal microbiome.
Materials and Methods. An interventional cross-sectional comparative study with 148 women was conducted. Depending on the present or absent of pathognomonic complaints and clinical signs of vulvovaginal atrophy (VVA), 113 postmenopausal patients were divided into 3 clinical groups: group 1 – 42 patients with VVA and reported subjective clinical symptoms and complaints; group 2 – 36 patients with VVA, visual signs of the atrophic process and no subjective clinical symptoms and complaints; group 3 – 35 healthy postmenopausal women without VVA signs. Control group consisted of 35 healthy women of reproductive age. The study used electrochemiluminescence immunoassay (ECLIA) to determine the level of blood plasma estradiol, molecular biological analysis (real-time polymerase chain reaction) – to study the vaginal microflora using the Femoflor-16 method. An assessment of epitheliocyte nucleus electrokinetic activity (ENEA) was carried out according to V.G. Shakhbazov et al. (1986) microelectrophoresis method, as well as an immunohistochemical (IHC) study of vaginal wall biopsies – to determine ERα expression using monoclonal antibodies as well as visualization systems and assessment conducted by Allred system.
Results. Our data showed that the pH of vaginal secretions increases from control group to groups with VVA, indicating a decreased acidity. In group 4 (reproductive age women), the pH was 3.89, significantly lower than in other groups (p < 0.001). In group 3 (postmenopause without VVA), the pH was higher than in control, but lower than that of in group with VVA (p < 0.001). Groups 1 and 2 (with VVA) have the highest pH, with group 1 (symptomatic) being higher than in group 2 (p < 0.001). In addition, there were also data obtained on microbiota state in the studied patients. All women (100.0 %) from group 1 had severe dysbiosis; in group 2, 25 % had severe dysbiosis, and 75 % had moderate dysbiosis. In group 3, individuals were distributed roughly equal proportions: normocenosis and normocenosis with signs of dysbiosis in 42.8 %, and 14.2 % with moderate dysbiosis. The maximum estradiol concentration in control group was 161.7 pg/ml, significantly higher than the others (p < 0.001). No significant differences between the groups with VVA were found. The ERa level decreased in groups with VVA: in asymptomatic vs. symptomatic patients with VVA, it was higher (p < 0.001). Women without VVA had the highest ERa level. ENEA decreased from control (53.9 %) to groups with VVA, especially in symptomatic subjects (up to 3.88 %). In patients from group 3, it was higher than in study groups with VVA (p < 0.001). Statistical analysis has shown that absolute normocenosis is associated with higher ENEA level compared to dysbiosis. The high correlation between ERa and ENEA shows that such indicators are interconnected and closely related to mucosal condition. The regression model showed that estradiol level and epithelial parameters were important for control group, while ENEA level and acidity dominated in VVA groups.
Conclusion. ENEA is a sensitive and non-invasive marker closely related to vaginal microbiota state. Its magnitude decreases in microbiota disorders and reaches 41.2 % in absolute normocenosis, mirroring a good mucosal condition. In postmenopause, even a conditional normocenosis is accompanied by ENEA decreased down to 35.2 %, which may suggest preclinical changes. With moderate dysbiosis, the indicators decrease by 3–4 times, and with severe dysbiosis – by more than 15 times, indicating seriously altered homeostasis. Statistical inter-group significance confirms the ENEA ability to objectively assess the degree of microbiological disorders. A level below 35 % highlights deviation from normal range, even without clinical symptoms. Magnitude of 2–10 % indicate severe dysbiosis requiring correction. Altered relationship between the parameters may suggest severity of the process and portend a poor response to treatment. Intensive combination therapy is recommended for patients with symptomatic VVA. With "silent" atrophy, therapy aimed at improving epithelial condition is sufficient, without significant changes in the hormonal background. Evidence suggests that preventive maintenance of microflora and acidity is important in postmenopausal women. For the first time, it is proposed to use ENEA as a parameter that bridges molecular disorders and clinical as well as microbiological manifestations of VVA, which lay a foundation for novel stratification and diagnosis system as well as differentiated treatment depending on regulatory relationships at the tissue level.
What is already known about this subject?
► Uterine fibroids are a common indication for surgery in reproductive-aged women, and organ-preserving approaches have been increasingly prioritized to maintain fertility potential.
► Laparoscopic myomectomy is an effective minimally invasive alternative to laparotomy, but intraoperative bleeding remains a major factor affecting surgical safety.
► Various vascular control techniques, including temporary uterine artery occlusion, are used to reduce bleeding, though clinical evidence on their effectiveness has been extensively accumulated.
What are the new findings?
► Transient uterine artery occlusion significantly reduced intraoperative blood loss compared with standard laparoscopic myomectomy.
► The occlusion technique did not prolong operative time and showed no increased early postoperative complications.
► The findings support safe implementation of the technique in reproductive-aged patients without adverse perioperative outcomes.
How might it impact on clinical practice in the foreseeable future?
► The method may serve as an adjunct strategy to reduce surgical risks during fertility-preserving procedures.
► Reduced blood loss may lower transfusion rates and facilitate faster postoperative recovery.
► These results support broader incorporation of transient uterine artery occlusion into minimally invasive gynecologic surgery standards.
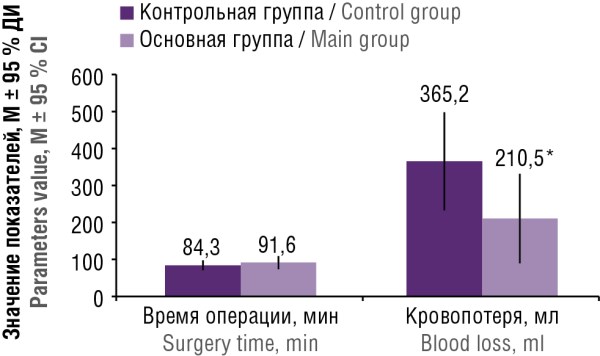
Aim: to evaluate the clinical efficacy of laparoscopic myomectomy using transient uterine artery occlusion in reproductive age patients with symptomatic uterine fibroids.
Materials and Мethods. The prospective comparative study included 20 women randomly assigned to two groups: standard laparoscopic myomectomy (n = 10) and laparoscopic myomectomy with transient uterine arteries occlusion (n = 10). The duration of the operation, the volume of intraoperative blood loss, the dynamics of hemoglobin levels, the duration of hospitalization, and the frequency of complications were evaluated.
Results. Both groups were comparable in baseline clinical and demographic characteristics. In main group, there was a significant decrease in intraoperative blood loss (210.5 ± 195.4 ml vs. 365.2 ± 214.1 ml; p = 0.03), while the duration of surgery and the level of postoperative hemoglobin did not differ significantly. Most of the interventions were completed by laparoscopic access without conversion, and frequency of early complications was comparable in both groups.
Conclusion. Transient occlusion of the uterine arteries during laparoscopic myomectomy improves the safety of the intervention by reducing blood loss and does not increase the risk of complications. The practical significance implies that the use of this technology can contribute to safer operations and preserve patients’ reproductive health. Thus, positively contributes to improving current gynecological surgery.
What is already known about this subject?
► Iron deficiency anemia and latent iron deficiency are highly prevalent among women of reproductive age in the Russian Federation and worldwide.
► Iron deficiency is associated with menstrual disorders, particularly menorrhagia, creating a "vicious cycle".
► Folic acid acts in synergy with iron in erythropoiesis and homocysteine metabolism, but regional data on combined deficiency are limited.
What are the new findings?
► For the first time, data on the high prevalence of combined iron deficiency (34.4 % – latent, 27.4 % – manifest) and folate deficiency (55.2 % overall) in women aged 20–25 years in the Republic of Bashkortostan are presented.
► Unbalanced nutrition (inadequate iron intake – in 83.9 %, vegetarian/vegan diet – in 15.2 %) is shown to be the main contributor to the development of such deficiencies in the region.
► A 3-month combined therapy with ferrous fumarate and folic acid proved to restore not only hemoglobin (in 95.2 %) but also iron depots (ferritin in 84.7 %) and folate status (in 100,0 %).
How might it impact on clinical practice in the foreseeable future?
► Regional screening for ferritin and folic acid in women of early reproductive age, especially those with menstrual irregularities, is advisable.
► The use of combined iron and folic acid supplements for preconception care is recommended given the high prevalence of combined deficiency in the region.
► Active correction of dietary habits among young women (increased intake of meat, fish, vegetables) is required for primary prevention of deficiency states.
Introduction. Iron deficiency conditions and folate insufficiency are highly prevalent among women of reproductive age in the Russian Federation and may adversely affect menstrual and reproductive function. Regional prevalence patterns and the effectiveness of combined correction for such deficiencies in the Republic of Bashkortostan remained understudied.
Aim: to assess the prevalence of iron and folic acid deficiency, associated dietary and gynecological risk factors, as well as the effectiveness of 3-month combined therapy with ferrous fumarate and folic acid in women of early reproductive age.
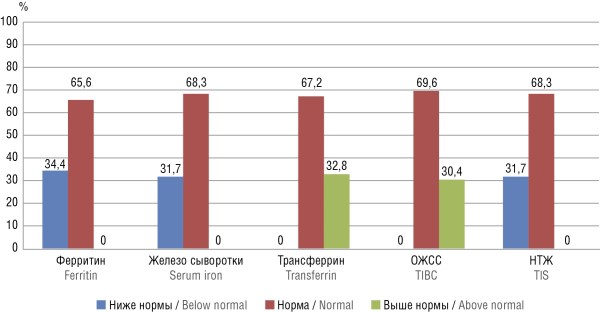
Materials and Methods. A prospective cohort study was conducted involving 372 women aged 20–25 years residing in the Republic of Bashkortostan. Actual nutrition was assessed (My Healthy Diet software), and menstrual blood loss was evaluated using the Mansfield–Voda–Jorgensen scale. Serum levels of ferritin, serum iron, total iron-binding capacity (TIBC), transferrin, transferrin iron saturation coefficient (TIS), folic acid, as well as complete blood count were measured. Women with iron deficiency received combined therapy – 163.56 mg ferrous fumarate (equivalent to 50 mg iron) + 540 µg folic acid (equivalent to 500 µg dry matter) for 3 months.
Results. Latent iron deficiency (ferritin < 15 µg/L) was detected in 34.4 %; 28.5 % had early latent iron deficiency (ferritin = 15 µg/L and changes in other ferrokinetic markers: decreased serum iron, TIS or increased transferrin and TIBC); the overall prevalence of iron deficiency signs was in 62.9 %. Manifest iron deficiency anemia (hemoglobin < 120 g/L) was detected in 27.4 %, folic acid deficiency (< 3 ng/mL) – in 23.7 %, and probable deficiency (3.0–5.9 ng/mL) – in 31.5 % of women. Inadequate iron intake (< 18 mg/day) was observed in 83.9 % of participants. Iron deficiency was associated with menorrhagia, abnormal uterine bleeding, and premenstrual syndrome. After 3 months of therapy, hemoglobin normalization was achieved in 95.2 %, ferritin normalization in 84.7 %, and serum folate normalization in 100,0 % of re-examined patients.
Conclusion. High prevalence of iron and folic acid deficiency associated with menstrual disorders and poor nutrition was found in women of early reproductive age in the Republic of Bashkortostan. Three-month combined therapy with ferrous fumarate and folic acid demonstrated high clinical and laboratory effectiveness.
What is already known about this subject?
► Preeclampsia (PE) is associated with long-term metabolic and endocrine disorders in offspring, including an increased risk of obesity and cardiovascular disease.
► The impact of adverse intrauterine factors on adolescent girls health is mediated through perinatal programming mechanisms and may manifest during puberty.
► Data regarding maternal PE effects on the reproductive development in paired daughters are limited and controversial, particularly regarding age at menarche and hormonal profile.
What are the new findings?
► Daughters born to mothers with PE experience menarche 1 year earlier and have a 1.8-fold higher prevalence of dysmenorrhea compared to control group.
► A bimodal body mass index distribution was observed in this group: underweight and obesity are 3 and 1.5 times more common, respectively, than in control group.
► Based on clinical and anamnestic data, a computer program was developed to predict menstrual cycle disorders in girls born to mothers with PE.
How might it impact on clinical practice in the foreseeable future?
► Girls born to mothers with PE should be identified as a risk group for menstrual dysfunction and metabolic disorders.
► Early dynamic follow-up assessing menstrual cycle, body mass index, and hormonal status in adolescence is recommended.
► These findings may serve as a basis for developing personalized preventive programs and screening approaches in pediatric gynecology.
Introduction. Complicated pregnancy and delivery pose risks not only to maternal health but also to the offspring in later life. Preeclampsia (PE) has long-term effects on child development, increasing the risk of metabolic and endocrine disorders. However, studies investigating the impact of PE on the reproductive health in adolescent girls are limited, and existing data remain controversial, underscoring the relevance of the current study.
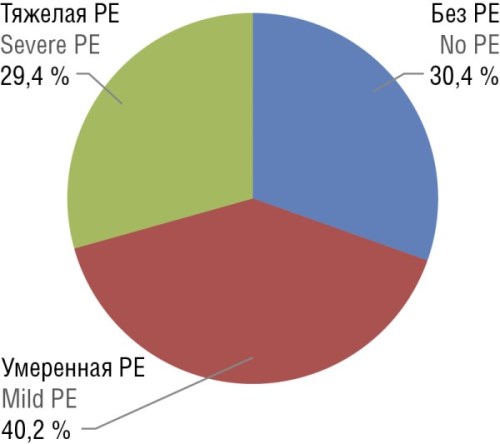
Aim: to assess the reproductive health and metabolic profile in adolescent girls depending on maternal PE during pregnancy and childbirth.
Materials and Methods. An ambispective cohort study was conducted. A total of 1,706 delivery records of women who gave birth to female infants in 2006, 2007 and 2008 were analyzed. From these, 184 adolescent girls who met the inclusion criteria were selected: singleton full-term spontaneous pregnancy, presence or absence of maternal PE, and live-born fullterm females delivered between 2006 and 2008. Participants were divided into two groups: main group – 128 girls born to mothers with moderate or severe PE, control group comprised 56 girls whose mothers had an uncomplicated pregnancy and delivery. A retrospective analysis of obstetric records and a prospective clinical assessment of adolescent girls were performed, including anthropometric evaluation with calculated standard deviation score (SDS) of body mass index (BMI), assessed menstrual and reproductive function, hormonal profiling, and ultrasound examination of the pelvic organs and mammary glands.
Results. In the main group, a higher prevalence of dysmenorrhea (p = 0.027) and earlier age at menarche (p = 0.001) was observed compared to control group. At the same time, no significant inter-group differences in menstrual cycle regularity, menstrual blood loss, or time to cycle establishment (p > 0.05) were found. Evaluation of physical development revealed significant differences in BMI category distribution (p = 0.031). In main group, both underweight (20.3 % vs. 7.1 % in controls) and obesity (10.9 % vs. 7.1 %), including severe forms (class III and morbid obesity), were more frequently observed; the latter were absent in control group. Among girls in main group, fetal growth restriction (FGR) was observed significantly more frequently – 26.6 % vs. 0.0 % in controls, (p < 0.001), and both birth weight and birth length were significantly lower (p = 0.002 and p < 0.001, respectively). Incomplete menstrual cycle maturation (14.1 % vs. 10.7 %) and prolonged cycle establishment (> 3 years: 4.7 % vs. 0,0 %) tended to be higher in the main group although the difference was not statistically significant (p = 0.176).
Conclusion. Maternal pregnancy complicated by preeclampsia is associated with altered reproductive health and metabolic profile in adolescent girls born to mothers with PE more frequently exhibiting primary dysmenorrhea, earlier menarche, and deviations in physical development such as bimodal distribution of BMI categories (increased prevalence of both underweight and obesity). These findings indicate a high-risk of menstrual dysfunction and metabolic disorders in girls born to mothers with PE, supporting a need for follow-up by a pediatric and adolescent gynecologist as well as development of personalized early prevention strategies.
REVIEW ARTICLES
What is already known about this subject?
► Compared to general population, patients with malignant neoplasms have a markedly higher risk of thrombotic complications, whereas their development is associated with poorer prognosis and changes in treatment strategy.
► The prothrombotic state in malignant neoplasms is driven by activation of the hemostatic system, endotheliopathy, platelet-leukocyte interactions, inflammatory responses as well as locally disturbed blood flow.
► Thrombosis at atypical sites requires an extended diagnostic work-up, including exclusion of occult malignancy or myeloproliferative neoplasms, as well as assessment for antiphospholipid syndrome, drug-associated factors, infectious or inflammatory triggers.
What are the new findings?
► It is reasonable to consider cancer-associated thrombosis as a continuum of arterial and venous thrombotic complications, including atypical and rare locations, rather than a pathology solely resulting in deep vein thrombosis and pulmonary embolism.
► An atypical thrombosis location has independent diagnostic significance, as it may point at occult malignancy, myeloproliferative neoplasm, antiphospholipid syndrome, or treatment-associated vascular injury.
► Clinical assessment of such thrombotic events should take into consideration not only tumor activity, but also ongoing anticancer therapy, endotheliopathy, infectious and immune-mediated triggers, bleeding risk, and potential drug-drug interactions.
How might it impact on clinical practice in the foreseeable future?
► Computed tomography and magnetic resonance imaging in cancer patients may be used more actively not only to assess dynamics of tumor process, but also to targeted detection of asymptomatic thrombosis at atypical sites.
► Preliminary risk for developing not only venous thromboembolism but also arterial thrombosis may be assessed more broadly while applying endocrine, targeted, antiangiogenic, and immunotherapy.
► Secondary prevention following atypical thrombosis may become more personalized, taking into account thrombosis location, tumor activity, planned treatment, recurrence risk as well as safety of long-term anticoagulant therapy.
Cancer-associated thrombosis is traditionally viewed mainly in the context of venous thromboembolism, however, the spectrum of thrombotic complications is markedly broader in patients with cancer. Apart from deep vein thrombosis and pulmonary embolism, it may include arterial thrombosis, cerebral venous thrombosis, splanchnic vein thrombosis, ovarian and renal vein thrombosis, as well as treatment- and immune-associated thrombotic disorders. The aim of this review is to discuss rare forms and atypical sites for cancer-associated thrombosis by covering their clinical significance, pathogenetic basis, association with anticancer therapy as well as concomitant prothrombotic conditions. The article discusses the main mechanisms underlying tumor-associated hypercoagulability, including the role for endothelial dysfunction, platelet activation, neutrophil extracellular traps, and thromboinflammation. Special attention is paid to arterial thrombosis, breast cancer therapy, cerebral venous thrombosis, abdominal vein thrombosis, COVID-19-associated coagulopathy as well as vaccine-induced immune thrombotic thrombocytopenia. Timely recognition of such conditions requires a multidisciplinary approach, proper imaging, and assessment of tumor-, patient-, and treatment-related risk factors.
What is already known about this subject?
► Prediction of preeclampsia (РЕ) and obstetric bleeding improves when multiparametric models combine clinical history, laboratory data and instrumental markers.
► For РЕ, blood pressure, maternal risk factors, uterine artery Doppler findings and placental biomarkers are the most consistent contributors.
► Most published models rely on retrospective datasets, while limited external and prospective validation reduces reproducibility and transportability.
What are the new findings?
► Not only models for predicting PE were compared, but also algorithms for assessing the risk of obstetric hemorrhage at the peripartum and preoperative stages.
► Best performance was generally achieved when routine laboratory data and, for РЕ, first-trimester screening markers were added to basic clinical variables.
► For bleeding, models based on electronic medical records and preoperative data in patients with placenta previa and placenta accreta spectrum (PAS) appear to be the most promising.
How might it impact on clinical practice in the foreseeable future?
► These algorithms may complement existing screening pathways by identifying women who need intensified surveillance or additional assessment.
► Bleeding-risk models could improve planning of referral, blood products, multidisciplinary teams and operating-room readiness.
► Implementation will require standardized reporting, local calibration and independent validation before integration into routine digital clinical systems.
Aim: to compare the predictive performance of artificial intelligence (AI) and machine learning (ML) models trained on multiparametric datasets for the prediction of preeclampsia (РЕ) and obstetric hemorrhage.
Materials and Methods. This systematic review was conducted in accordance with the PRISMA guidelines. PubMed and Cochrane Central databases were searched for studies published between 2015 and 2025. We included studies applying AI/ML with ≥ 2 predictors/data modalities and reporting outcomes related to РЕ/eclampsia or obstetric hemorrhage (including postpartum hemorrhage). Risk of bias was assessed using Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool and the Newcastle–Ottawa Scale (NOS).
Results. Twenty-eight studies were included (18 on РЕ and 10 on hemorrhage). Most common algorithms were gradient boosting methods, random forests, XGBoost, and neural networks were the most common algorithms. For preeclampsia, stronger performance was more consistently reported when maternal risk factors were combined with blood pressure features and first-trimester screening components (uterine artery Doppler and placental biomarkers). For hemorrhage prediction, models based on electronic health records and preoperative clinical and laboratory variables, including risk stratification in placenta previa/placenta accreta spectrum (PAS), appeared particularly relevant. The evidence base is limited by predominantly retrospective designs and insufficient external/prospective validation, which undermines model transportability across settings and over time.
Conclusion. AI supported by multiparametric monitoring shows promise for predicting РЕ and obstetric hemorrhage; however, real-world implementation requires standardized reporting, external validation, and ongoing calibration monitoring.
What is already known about this subject?
► Placenta-associated complications (РАС) – preeclampsia (PE), fetal growth restriction (FGR), intrauterine fetal death (IUFD) as well as placental abruption (PA) are linked to impaired spiral artery remodeling and hemostasis activation, providing a rationale for anticoagulant therapy.
► Previous systematic reviews yielded conflicting results due to the inclusion of patients with thrombophilia and the use of varying therapeutic approaches.
What are the new findings?
► The study focuses on a cohort of high-risk women without thrombophilia and venous thromboembolism allowing for evaluation of low-molecular-weight heparins (LMWHs) effect beyond its classical indications and clarifying its role specifically in PAC prevention.
► An analysis of various placenta-associated outcomes was conducted, revealing the heterogeneous LMWHs efficacy: a pronounced effect on certain complications while no effect on others, highlighting the heterogeneity of their pathogenesis.
► The limitations of the existing evidence base have been highlighted, including the heterogeneity of studies and potential publication bias, which underscores the need for more standardized and large-scale randomized trials.
How might it impact on clinical practice in the foreseeable future?
► The data obtained can serve as a basis for personalized LMWHs prescription to patients with a high risk of PE, IUFD and PA, especially with a complicated obstetric history.
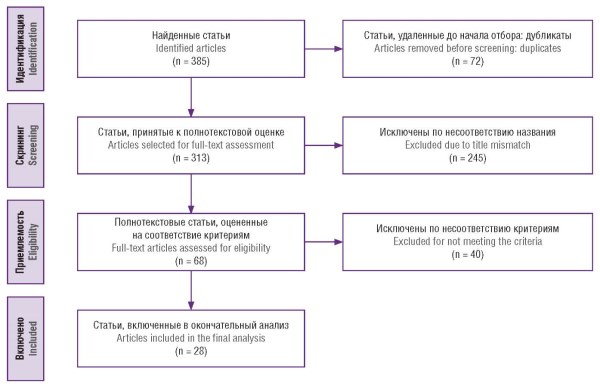
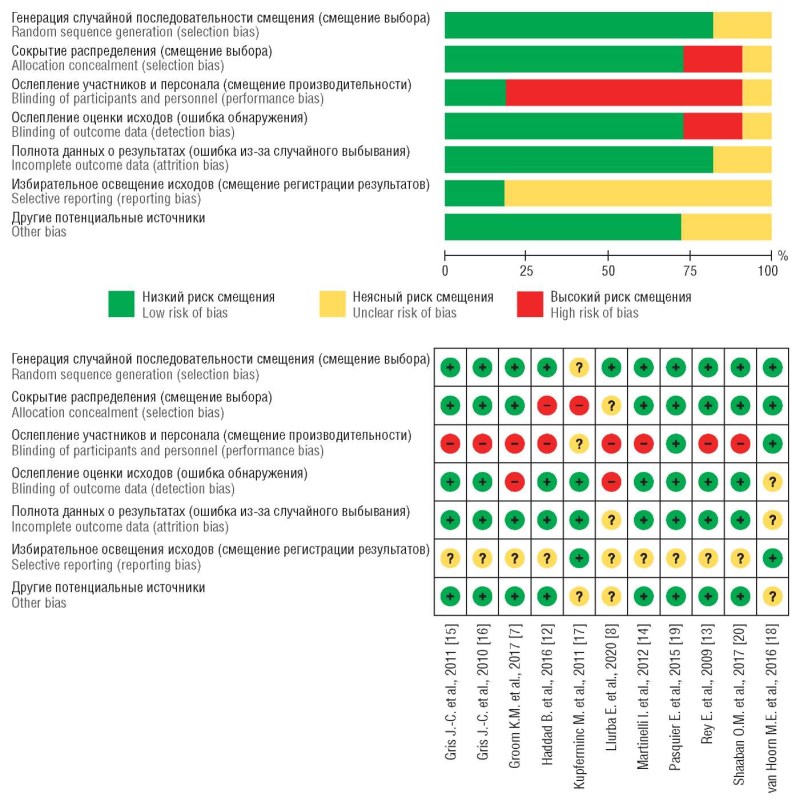
Aim: to evaluate the effectiveness of low-molecular-weight heparins (LMWHs) in preventing placenta-associated complications (РАС), such as preeclampsia (PE), fetal growth restriction (FGR), intrauterine fetal death (IUFD) and placental abruption (PА), in women at high risk for these complications but without thrombophilia or thromboembolic complications, based on a review and meta-analysis of publications released within the last twenty years.
Materials and Methods. A search for relevant randomized controlled trials was conducted in electronic databases (PubMed/ MEDLINE, Embase, Web of Science, etc.) spanning from 2005 to 2025. The meta-analysis included 11 trials involving a total of 1965 women. PE, FGR, IUFD, and PA were considered as the primary outcomes. Fixed-effects models were used for analysis, and the results were presented as risk ratios with 95 % confidence intervals.
Results. LMWHs use was associated with a reduced IUFD risk (0.69 [0.55; 0.86]; p = 0.001), PA (0.67 [0.52; 0.86]; p =0.002), and PE occurrence (0.66 [0.52; 0.85]; p = 0.001). No significant effect of LMWHs use on FGR risk was found (0.93 [0.69; 1.25]; p = 0.62). Considerable heterogeneity (I2 > 60 %) was observed while analyzing IUFD, PE and PA. Funnel plot assessment did not rule out a potential risk of publication bias and requires further investigation.
Conclusion. Prophylactic LMWHs use in women at high risk for РАС without thrombophilia may reduce the incidence of complications such as PE, IUFD, and PA. These findings indicate the need for multicenter studies with detailed analyses to identify patient cohorts where prophylactic LMWHs use for complication prevention provides a clear clinical and pathogenetic rationale.
What is already known about this subject?
► Deep infiltrating endometriosis (DIE) profoundly impairs quality of life due to chronic pain, a high risk of infertility, and its potential for malignant transformation.
► Both ovarian and extra-ovarian endometriosis-associated cancer is characterized by aggressive behavior most often being diagnosed at advanced stages.
► Differential diagnosis between DIE and endometriosis-associated cancer is challenging due to overlapping clinical, morphological, and molecular features.
What are the new findings?
► This article provides an overview of current and most informative approaches to the differential diagnosis of DIE and endometriosis-associated cancer.
► Key molecular genetic markers associated with malignant transformation in DIE have been identified and summarized.
► The potential for machine learning algorithms to detect malignant transformation using MRI data is demonstrated.
How might it impact on clinical practice in the foreseeable future?
► Systematization of diagnostic approaches may lay a foundation for developing a unified algorithm for differential diagnosis DIE and endometriosis-associated cancer.
► Implementing integrative diagnostic algorithm may improve early detection rates of endometriosis-associated cancer.
► Integration of artificial intelligence into the diagnostic process will enhance clinical decision-making support.
Deep infiltrating endometriosis is a socially significant condition that markedly reduces patients’ quality of life due to chronic pain syndrome and a high risk of infertility. In recent years, increasing evidence has emerged regarding the malignant transformation of the disease, with the malignant foci developing predominantly in the ovaries, as well as in extra-ovarian locations. The similarity of clinical manifestations, morphological characteristics, and molecular alterations between benign and malignant disease forms markedly complicates differential diagnosis. This article summarizes current concepts regarding the criteria for distinguishing deep infiltrating endometriosis from endometriosis-associated cancer. It highlights the limited evidence base and the need to develop standardized integrative approaches to improve diagnostic accuracy and stratification of oncological risk in this group of patients.
What is already known about this subject?
► Term neonatal heart rate (HR) “norms” (often 120–140 bpm) are widely used in clinical practice, yet their historical origins and validity are rarely examined systematically.
► Neonatal HR varies with transitional physiology, sleep/awake state, and measurement conditions; rigid cutoffs without context may mislead clinical interpretation.
► Various recording methods (auscultation/palpation, electrocardiogram, Holter monitoring) yield non-equivalent HR estimates – particularly at extremes – limiting transferability of “normal” values across measurement modalities.
What are the new findings?
► This work uniquely integrates a 1710–2025 historical bibliographic review with a PRISMA systematic review, linking evolving “normal” HR concepts to measurement methodology.
► Mean HR values in healthy term newborns appear similar across historical periods, while maximal HR is higher in contemporary instrumental studies; differences largely track measurement modality.
► Marked physiological variability including very low and very high values makes rigid reference thresholds unreliable without considering postnatal age and clinical context.
How might it impact on clinical practice in the foreseeable future?
► The study encourages contextual HR interpretation by age, state (sleep/awake), and measurement modality, reducing the risk of overdiagnosis bradycardia and tachycardia.
► Supports standardized delivery-room assessment: clinical HR counting remains useful but requires correct technique and awareness of expected variability.
► Justifies prospective studies with parallel clinical counting, pulse oximetry, and electrocardiogram to refine practical reference values and monitoring algorithms.
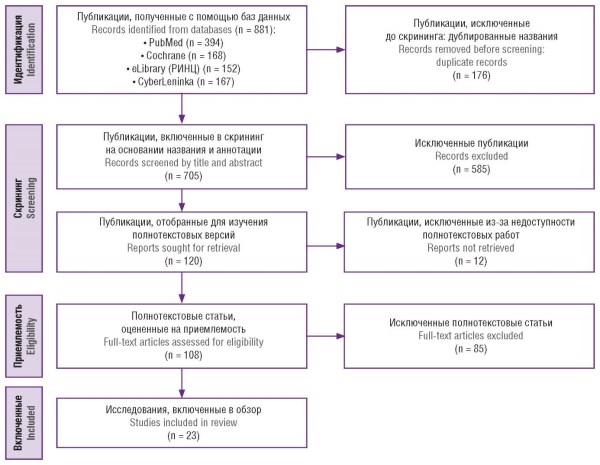
Aim: to systematically summarize published findings on reference (normative) heart rate (HR) magnitude in healthy term newborns during the first 7 days of life and to examine HR variability with respect to measurement method and age at assessment; additionally, to provide a historical bibliographic perspective on how neonatal HR norms evolved.
Materials and Methods. We conducted a PRISMA-reported systematic review for the contemporary evidence base and a separate historical bibliographic component. Searches were performed in PubMed/MEDLINE, Cochrane Central, eLibrary, and CyberLeninka. After deduplication, 705 unique records were screened; 23 studies were included in the systematic component. Thirteen historical sources were additionally included (overall period covered 1710–2025). Data extraction followed a standardized form; methodological quality for the systematic component was appraised using the JBI checklist. All quantitative comparisons were performed at the study level and interpreted as exploratory.
Results. Historical sources report a wide HR range predominantly obtained by clinical assessment (e.g., 72–172 bpm). Contemporary instrumental studies confirm substantial physiological variability in healthy term newborns, with reported HR values spanning from 55 bpm up to 240 bpm. Mean HR values appear broadly comparable across source groups (approximately 136–140 bpm). However, maximal HR values are lower in historical sources compared with contemporary instrumental data, and marked differences exist across groups in HR measurement methods.
Conclusion. Reference HR values in healthy term newborns exhibit wide physiological variability, limiting the use of rigid thresholds without considering postnatal age, functional state, and measurement modality. While mean HR values remain broadly comparable across historical periods, extreme values (particularly maximal HR) and measurement approaches differ substantially.
What is already known about this subject?
► Preeclampsia (PE) is associated with higher future risk of chronic hypertension, coronary ischemia, and stroke.
► PE pathogenesis involves a two-stage process: placental hypoperfusion followed by systemic endothelial dysfunction.
► In PE, hemostasis activation (elevated factor VIII, D-dimer) and chronic vascular inflammation are observed.
What are the new findings?
► Neutrophil extracellular traps (NETs) are proposed as a central arm uniting placental ischemia, oxidative stress, hypercoagulability, and endothelial damage in PE.
► Recurrent PE causes cumulative vascular damage, transitioning acute thromboinflammation into chronic cardiovascular disease.
► Low-molecular-weight heparins (LMWHs) have pleiotropic effects (NET suppression, complement modulation) beyond anticoagulation per se.
How might it impact on clinical practice in the foreseeable future?
► Women with recurrent PE should undergo early cardiovascular screening especially with HELLP syndrome, eclampsia, fetal growth restriction.
► LMWHs may become a preferred recurrence prevention strategy in PE patients with thrombophilia due to anti-inflammatory and endothelial-protective effects.
► Assessing NETs and thromboinflammatory markers may help stratify women for long-term cardiovascular risk.
Preeclampsia (PE) is not only an acute obstetric complication but also a significant factor in long-term cardiovascular risk. This article analyzes the pathogenetic mechanisms linking recurrent severe PE with the development of chronic arterial hypertension, coronary heart disease, stroke, and heart failure in the long-term. Particular attention is paid to the two-stage PE model, as well as the key role for immune-inflammatory responses, oxidative stress, and hemostatic disorders. Recurrent PE is shown to cause cumulative damage to the vascular bed, transforming acute inflammation into chronic cardiovascular pathology. Neutrophil extracellular traps collectively resulting in innate immune activation, hypercoagulability, and endothelial damage, play a central role in the pathogenesis. Current approaches to preventing recurrent PE such as acetylsalicylic acid, calcium supplements, and low-molecular-weight heparins are discussed.
What is already known about this subject?
► Despite significant advances in assisted reproductive technologies (ART), the effectiveness of a single in vitro fertilization (IVF) cycle remains limited, with failure rates reaching 50–60 %, highlighting the need for improved prognostic tools.
► Morphological embryo assessment and morphokinetic analysis are widely used; however, their predictive accuracy is limited. Preimplantation genetic testing shows benefit solely mainly in selected clinical groups.
► Accumulating evidence suggests the role for oxidative stress, immune dysregulation, and molecular alterations in follicular fluid and the endometrium, although their clinical implementation remains sparse.
What are the new findings?
► This review integrates the data on redox markers, microRNAs, cell-free DNA, and immunological parameters into a unified molecular stratification concept in ART programs.
► It provides a comparative analysis of the predictive performance for individual biomarkers, including sensitivity, specificity, and AUC values, allowing assessing their clinical relevance.
► The article emphasizes the transition from isolated biomarker evaluation to integrated multifactorial models supported by multi-omics approaches and digital analytical tools.
How might it impact on clinical practice in the foreseeable future?
► Comprehensive molecular profiling may improve embryo selection and optimize transfer strategies in IVF programs.
► Redox and immunological assessment could help identify patients at increased risk of implantation failure and guide targeted interventions before subsequent cycles.
► Integration of laboratory biomarkers with clinical parameters and machine learning algorithms may facilitate the development of personalized infertility management strategies.
Despite substantial advances in assisted reproductive technologies (ART), the proportion of unsuccessful in vitro fertilization cycles remains considerable, highlighting the need for additional prognostic tools. In recent years, increasing attention has been directed toward molecular and immunological markers that reflect oocyte competence, embryo developmental potential, endometrial receptivity, and the patient’s systemic inflammatory status. This review summarizes current evidence regarding the diagnostic and predictive value of biomarkers identified in follicular fluid, peripheral blood, and endometrial tissue. Particular emphasis is placed on oxidative stress markers (malondialdehyde, advanced oxidation protein products), antioxidant enzymes (including glutathione peroxidase), microRNAs and other non-coding RNAs, as well as immunological parameters such as cytokines, complement components, and immune cell subsets. Data on circulating cell-free DNA as an indicator of follicular microenvironment status are also discussed. Available evidence suggests that disturbances in redox balance and alterations in local immune regulation may be associated with impaired embryo quality and reduced implantation rates. However, substantial methodological heterogeneity, small sample sizes, and the lack of standardized assessment protocols limit the clinical applicability for many proposed biomarkers. Integration of molecular markers with clinical parameters, supported by multi-omics approaches, offers promising opportunities for the personalization of ART strategies. Nevertheless, large prospective studies with robust validation and evaluation of cost-effectiveness are required before these biomarkers can be incorporated into routine clinical practice.
What is already known about this subject?
► Precancerous lesions and vulvar cancer remain significant challenges in gynecologic oncology due to increasing incidence rates, delayed diagnosis, and their substantial impact on patients’ quality of life.
► Traditional treatment methods for vulvar cancer are often accompanied by functional and psychosexual impairments, requiring development of organ-preserving approaches.
What are the new findings?
► Current data on the molecular mechanisms underlying the development of the pathology and the role for diagnostic methods in detecting precancerous lesions and vulvar cancer are summarized.
► Modern organ-preserving treatment approaches and rehabilitation strategies aimed at improving patients’ quality of life are presented.
How might it impact on clinical practice in the foreseeable future?
► Introduction of molecular and immune biomarkers may improve accuracy of early diagnosis and enable patient-oriented treatment strategies.
► Wider application of organ-preserving techniques may reduce the rate of postoperative complications and improve functional therapy outcomes.
Vulvar premalignant lesions and vulvar cancer represent a significant issue in modern gynecologic oncology. The importance of this problem is driven by the increasing incidence, the impact on patients’ quality of life, and the difficulty of early-stage diagnosis. In recent decades, understanding of the pathogenesis, classification, and treatment approaches for such pathologies has been dramatically changed. This review presents current data on the epidemiology, classification, molecular mechanisms of development, diagnostic methods as well as treatment of vulvar premalignant lesions and vulvar cancer. Special attention is paid to the role played by immunohistochemical markers, novel non-invasive diagnostic methods, and organ-preserving therapeutic approaches. Issues of secondary prevention, including HPV vaccination, as well as modern rehabilitation strategies aimed to improve patients’ quality of life are also outlined.
FROM HISTORY
The article presents a historical and scientific review regarding the development of concepts about interplay between malignant neoplasms and thrombotic complications. The evolution of views on cancer-associated thrombosis is outlined: from the first clinical observations by J.-B. Bouillaud and the classic description by Armand Trousseau to the modern concept of tumor-associated coagulopathy and thrombotic risk stratification. The significance of the works carried out by R. Virchow and T. Billroth for the transition from clinical observations to a pathogenetic understanding of thrombosis as well as H. Dvorak’s contribution to form insights into tumor as a “wound that never heals,” pathological angiogenesis, vascular permeability, and the role for vascular endothelial growth factor are demonstrated. Special attention is paid to emergence of clinical hemostasiology, including the studies by M.-M. Samama, the International Conference on Thrombosis and Hemostasis Issues in Cancer (ICTHIC), and the contribution of the Russian Z.S. Barkagan and A.D. Makatsariya scientific schools to investigating hemostatic disorders, thrombophilia, and thrombosis in cancer patients. The final stage of this historical timeline is associated with the works by A. Khorana and the transition to formalized risk assessment of venous thromboembolic complications in patients with malignant neoplasms. Such analysis allows cancer-associated thrombosis to be envisioned not only as a vascular complication related to tumor process, but also as a genuine manifestation of the complex crosstalk between the tumor, the hemostatic system, the endothelium, inflammation, anticancer treatment, and individual patient risk factors.
EVENTS



This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
ISSN 2500-3194 (Online)






































