


“Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) is a scientific and practical peer-reviewed journal for obstetricians, gynecologists and other experts in the area of women’s health. Our aims and priorities focus on scientific and information support to the members of the "professional community" in their pursuit of new ideas in obstetrics and gynecology research. In addition, the AGR journal proudly contributes to the continuing medical education (CME) of practitioners who specialize in various areas of women’s health including obstetrics, gynecology, in vitro fertilization (IVF) and assisted reproductive technology (ART).
“Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) was founded in 2007
The impact factor of this journal, as shown in the Russian Science Citation Index (RSCI) is among the highest for the periodicals on obstetrics, gynecology, perinatology and problems of women’s health. According to RSCI, the biennial impact factor was 0.509 in 2013, 0.810 in 2014, and 0.976 in 2015.
The journal publishes original articles on clinical and experimental studies, as well as reviews on obstetrics, gynecology, and human reproduction. Special attention is paid to publications on CME as well as historic aspects of obstetrics and gynecology. All manuscripts, both original research and literature reviews, are published upon a mandatory peer-review.
Languages: Russian, English
Periodicity: 6 issues per year.
The printed versions are distributed under the Creative Commons Attribution 4.0 License: full-text materials are freely available to the public in an open access repository.
Distribution of the printed version: Russia, the EurAsian Economic Community (EurAsEC) countries (Belarus, Kazakhstan, Kyrgyzstan, Tajikistan, Uzbekistan, Armenia, Moldova), Ukraine, Georgia.
The editorial board of “Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) includes leading scientists from Russia, Austria, Great Britain, Israel, USA, Croatia, Ukraine, Georgia, and Uzbekistan.
The editorial board of this journal maintains the policy of full compliance with all principles of publishing ethics. Our ethical standards and codes conform to those of top international science publishers.
All submitted materials undergo a mandatory double-blind peer review.
Media Certificate of Registration: ПИ №FS77-34885 of December 29, 2008.
ISSN 2077-8333 (Print)
ISSN 2311-4088 (Online)
By the decision of the Higher Attestation Commission (HAC) of Russia, “Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) is included in the "List of top peer-reviewed scientific journals and publications" where scientists seeking academic degrees are required to publish their results.
The “Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) journal appears in the Russian Universal Scientific Electronic Library (RUNEB) elibrary.ru and is also present in the database of the Russian Science Citation Index (RSCI). Concise versions of major articles from this journal are published by the All-Russian Institute for Scientific and Technical Information (VINITI). The journal is also indexed by "Ulrich's periodicals Directory" – a global information system of periodicals and continued publications.
Current issue
EDITORIAL
This editorial summarizes the materials from the first issue of 2026, united by the idea of moving toward predictive and personalized medicine in obstetrics and gynecology. Original research presents digital models for risk stratification of preterm birth and preeclampsia, neural network algorithms for selecting therapy for ovulation disorders, immunological and coagulation markers of placental complications, as well as data on long-term cardiometabolic risks after preeclampsia and factors preserving ovarian reserve. Review publications highlight current understanding of thrombosis pathogenesis in paroxysmal nocturnal hemoglobinuria, the role of natriuretic peptide in obstetrics and neonatology, immunocoagulation mechanisms of amniotic fluid embolism, the molecular basis of HPV-associated neoplasia, and fertility restoration strategies in women of late reproductive age. A clinical case of antenatal diagnosis of placenta accreta using modern ultrasound criteria is presented. The issue also includes retraction note due to identified unfair plagiarism, underscoring the editorial board's commitment to publication ethics. Taken together, the materials in this issue reflect contemporary developments in the specialty – risk stratification, personalized therapy, and the expansion of preventive care in obstetrics and gynecology.
ОRIGINAL ARTICLES
What is already known about this subject?
► Preterm birth (PTB) remains an unresolved global challenge in obstetrics, being the leading cause of neonatal mortality and childhood disability. Despite well-established risk factors (infections, cervical insufficiency, multiple gestation), the global PTB rate has persistently remained high (5–18 %). Existing preventive strategies have limited effectiveness, and the multifactorial nature of PTB complicates prediction using conventional statistical methods.
► In recent years, machine learning (ML) has been actively investigated for predicting obstetric complications, demonstrating strong potential in international studies. However, many existing models were developed on standardized English-language datasets and are not adapted to the realities of the Russia-wide healthcare system.
What are the new findings?
► This study represents an initial step toward a comprehensive PTB prediction tool tailored to Russian-language electronic health records (EHRs).
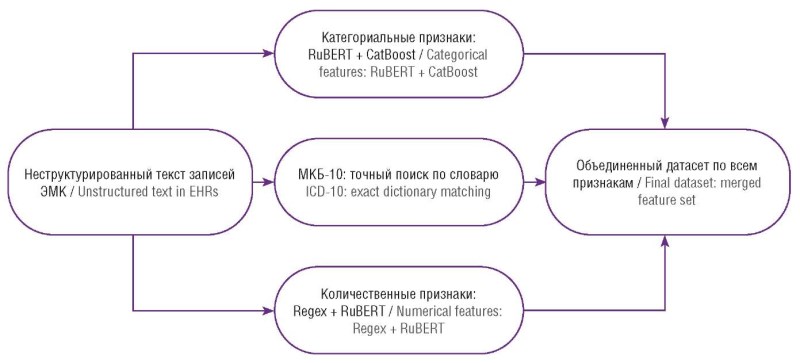
► The methodological novelty lies in the design and integration of a specialized NLP (natural language processing) model that automatically extracts 54 PTB-related clinical features from unstructured physician notes. This directly addresses a key barrier to leveraging real-world clinical data within domestic healthcare.
► A comparative evaluation of 14 ML algorithms showed that the algorithm based on gradient boosting CatBoost Сlassifier delivers the best performance, as confirmed by external validation. The article thus describes an end-to-end pipeline for automated analysis of routine clinical documentation to estimate PTB risk.
How might it impact on clinical practice in the foreseeable future?
► Implementing the proposed tool in routine medical care would enable automated PTB risk screening for every female patient based on data already contained in her EHR. Clinicians would gain an objective decision-support instrument for early identification of high-risk pregnancies and timely initiation of personalized preventive measures (e.g., progesterone the-
rapy).
► Integrating the system into medical information systems would allow automated high-risk alerts, helping optimize care pathways and management strategies. Over time, broader adoption could contribute to reducing PTB rates and improving perinatal outcomes in geographic regions deploying this technology.
Introduction. Preterm birth (PTB) remains one of the most serious complications of pregnancy, being the leading cause of neonatal mortality and contributing to long-term disability along with chronic morbidity in newborns, as well as imposing substantial socioeconomic costs. Despite preventive efforts, the global PTB rate has remained largely unchanged comprising 5–18 %, underscoring a need for developing more effective prediction tools to enable timely prevention.
Aim: using an independent sample to develop and validate a PTB risk-assessment tool based on machine learning (ML) and routinely collected clinical data retrieved from electronic health records (EHRs) of pregnant patients.
Materials and Methods. We analyzed a dataset of 10,000 de-identified EHRs entries containing 54 variables, including historical, clinical, laboratory, and instrumental (diagnostic/imaging) data. The predictive system comprised two interconnected ML components: (1) an NLP model based on RuBERT (а pre-trained ML model for processing Russian texts) for extracting PTB-relevant features from unstructured Russian-language clinical text, and (2) a downstream predictive ML model, for which 14 algorithms were benchmarked.
Results. The NLP model demonstrated high performance with a median sensitivity = 0.998, F1-score = 0.976, and AUC-ROC = 0.974. Among the ML algorithms, the algorithm based on gradient boosting – CatBoost Classifier (Categorical Boosting Classifier) achieved the best risk-prediction results: accuracy = 0.81, sensitivity (recall) = 0.87, precision = 0.76, F1-score = 0.81, and AUC-ROC = 0.82.
Conclusion. The developed model showed performance comparable to that of international counterparts, and validation confirmed its robustness to previously unseen data, indicating strong potential for use in routine clinical practice. This study represents the first step toward an integrated PTB risk-assessment solution combining NLP and ML. Future work will include incorporation of additional predictors (e.g., biochemical markers) and multicenter validation studies.
What is already known about this subject?
► About 20 % of reproductive age women are obese, and more than half of them experience menstrual cycle (MC) disorders, anovulation and infertility.
► Metformin is widely used to treat obese patients. However, its action is limited to its effect on carbohydrate metabolism. Metformin is not indicated for treatment of obesity.
► Positive results have been demonstrated by drugs based on myoinositol (MI) and D-chiroinositol (D-СI), general name – inositol, as insulin sensitizers, as well as agents for restoring the menstrual cycle and ovulation.
What are the new findings?
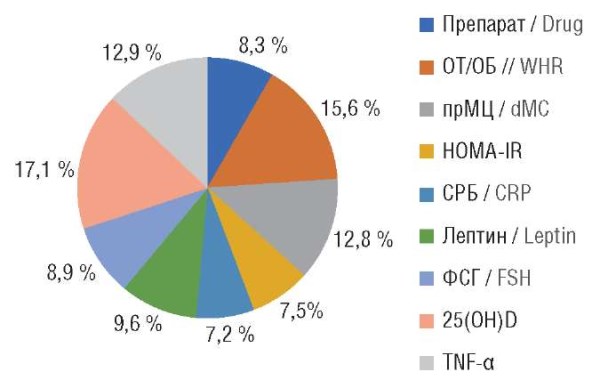
► The most significant parameters determining the restoration of ovulation were identified: intake of inositol or metformin, waist-to-hip ratio, MC duration, Insulin Resistance index (HOMА-IR), C-reactive protein, leptin, follicle-stimulating hormone, 25-hydroxycalciferol, tumor necrosis factor alpha.
► A model for predicting the onset of ovulation while using a specific drug was developed (sensitivity – 100 %, specificity – 80 %, accuracy – 93.8 %; area under the ROC curve – 0.985; p < 0.001).
How might it impact on clinical practice in the foreseeable future?
► A differentiated approach to select treatment modality is required based on certain predictors of carbohydrate and lipid metabolism disorders, hormonal status and other indicators.
► The developed prognostic model was used to create an online calculator, which allows for individual treatment selection for restoring ovulation in patients with obesity and oligo-/amenorrhea in routine clinical practice (accuracy – 91.7 %).
Introduction. Approximately 20 % of reproductive age women are obese, and more than half of them experience menstrual irregularities, anovulation, and infertility.
Aim: to determine predictors of ovulation restoration and to develop a model for individual treatment selection in patients with obesity and oligo-/amenorrhea based on neural network technology.
Materials and Methods. The prospective randomized controlled study included 80 women – patients with obesity and oligo-/amenorrhea, divided into 2 groups, who received the following therapy for 6 months: 40 patients (group I) – a combination of myoinositol, D-chiroinositol, folic acid and manganese, the other 40 patients (group II) – metformin. After treatment, patients from both groups were divided into two clusters based on the "anovulation/ovulation" criterion. Anthropometric parameters were determined, pelvic organs ultrasound was performed, laboratory tests (indicators of carbohydrate and fat metabolism, amino acids and peptides, hormonal status, blood cytokine levels, inflammation markers, and blood micronutrient composition) were performed. To create a model for predicting ovulation restoration, a multilayer perceptron procedure was used. The diagnostic value of the prognostic model was determined using ROC analysis.
Results. The average age of the patients was 27.9 ± 3.8 years, with the average body mass index (BMI) 33,4 [31.2; 34.0] kg/m2. The following parameters were identified as significant anovulation predictors using neural network analysis: waist-to-hip ratio (WHR), menstrual cycle duration, Homeostasis Model Assessment of Insulin Resistance (HOMA-IR), C-reactive protein, leptin, follicle-stimulating hormone, 25-hydroxycalciferol (vitamin D), and tumour necrosis factor alpha. Because these parameters reflect the metabolic profile in patients, interventions to restore ovulation should primarily be aimed at correcting it. The developed model for predicting the onset of ovulation has a sensitivity of 100 %, specificity of 80 %, accuracy of 93.8 %; the area under the ROC curve is 0.985 (p < 0.001), which allows to consider it sufficiently informative for specific drug selection. For practical purposes, an online calculator for individual drug selection has been developed (accuracy – 91.7 %).
Conclusion. An integrated approach based on neural network analysis of study parameters available for wide clinical practice is promising for predicting the onset of ovulation while using a specific drug due to its high information content.
What is already known about this subject?
► Chronic placental insufficiency (CPI) is a major contributor to fetal growth restriction (FGR), preeclampsia, and perinatal loss, especially in patients with adverse obstetric histories.
► Detected antiphospholipid antibodies (АРА) significantly associate with increased CPI risk and adverse pregnancy outcomes, even during preconception stages.
► Immune imbalance, particularly increased NK cells and B-lymphocytes, contributes to maternal-fetal immune tolerance and impaired trophoblast invasion.
What are the new findings?
► For the first time, a mathematical model based on immunological predictors for predicting CRF at pregnancy planning stage in women with complicated obstetric history has been developed.
► High diagnostic value of immunological markers – APA titers, B-lymphocytes, and NK cells for revealing patients with CPI risk before conception was demonstrated.
► The proposed model allows to stratify patients into risk groups with 85.7% sensitivity and specificity, which exceeds the performance indicators of existing diagnostic algorithms.
How might it impact on clinical practice in the foreseeable future?
► The model allows to early identify high-risk women before pregnancy for personalized preconception intervention.
► Introducing the algorithm into clinical practice will improve risk stratification and enable personalized pregnancy management strategies.
► Using the model can help to reduce the incidence of CPI, FGR and perinatal losses via early intervention and dynamic monitoring.
Introduction. Chronic placental insufficiency (CPI) is one of the leading causes of fetal growth restriction (FGR), perinatal loss, and complicated pregnancy. Currently, no validated methods for predicting CPI during pregnancy planning are available, which complicates high-risk patient stratification early and enabling timely prevention.
Aim: to develop a mathematical model for predicting CPI risk in women with a complicated obstetric history at the pre-pregnancy preparation stage.
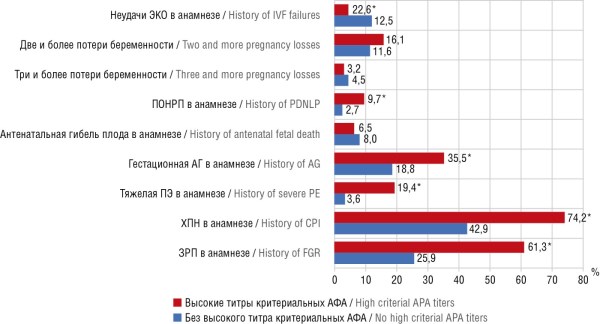
Materials and Methods. A retrospective clinical study assessing 462 patients with a complicated obstetric history was conducted. The outcomes of previous pregnancies, concomitant extragenital diseases, circulation of criterial (anti-β2glycoprotein and anti-cardiolipin antibodies, lupus anticoagulant) and non-criterial (anti-annexin 5, anti-phosphatidylserine, anti-phosphatidylinositol, anti-prothrombin, anti-human chorionic gonadotropin) antiphospholipid antibodies (APA), indicators of lymphocyte subpopulation composition, coagulation profile, and genetic thrombophilia were evaluated. Enzyme-linked immunosorbent assay, flow cytometry, ultrasound, and histological diagnostics were used. Binary logistic regression was applied to construct a prognostic model, and the diagnostic significance of the indicators was assessed using ROC curves.
Results. Detected APA high titers and/or lupus anticoagulant were associated with significantly elevated CPI incidence (63.1% vs. 4.6%; p < 0.001) and FGR (43.4% vs. 4.6%; p < 0.001). Immunological imbalance (increased percentage of B-lymphocytes and NK cells) increased CPI risk by 1.3–5.5 times. The constructed prediction model, which included indicators of immunological activity and comorbidity, demonstrated high accuracy: AUC = 0.89, sensitivity 85.7%, specificity 85.7%.
Conclusion. The developed mathematical model allows for highly accurate prediction of CPI risk developing in women with a complicated obstetric history even before pregnancy, which opens up avenues for personalized selection of preventive measures, including immunomodulatory therapy and dynamic monitoring, and contributes to lowering frequency of perinatal complications.
What is already known about this subject?
► Preeclampsia (РЕ) remains one of the leading causes for maternal and perinatal morbidity and mortality.
► Placental dysfunction is the key arm in РЕ pathogenesis.
► The complement system plays a crucial role in pregnancy-related immune regulation.
What are the new findings?
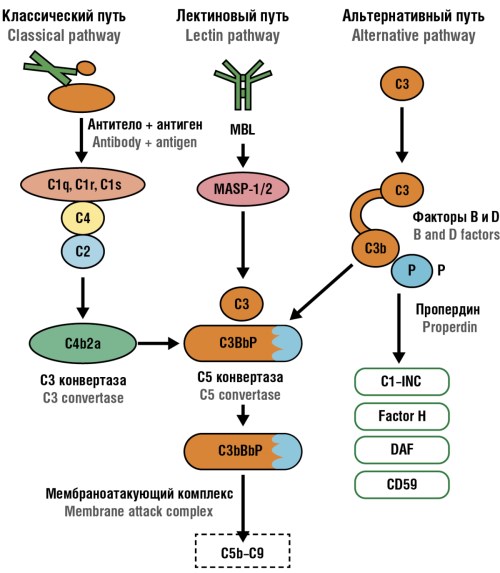
► Early-onset PE is characterized by predominantly increased C1q, mirroring locally activated classical complement pathway and placental dysfunction, whereas the late-onset PE is accompanied by elevated MAC (C5b–C9) level evidencing about complement terminal activation and systemic endothelial damage.
► Quantitative thresholds for C1q ≥ 250 ng/ml, C3a ≥ 615 ng/ml, and MAC ≥ 2717 mAU/ml were identified, associated with the risk of fetal growth restriction (FGR) and impaired uteroplacental blood flow, which may be used as potential biomarkers for complicated pregnancy.
► The inclusion of immunological indicators (C1q, C3a, MAC) in the risk assessment system allows for differentiating disease forms and predicting perinatal complications, opening up avenues for personalized prevention and therapy.
How might it impact on clinical practice in the foreseeable future?
► Quantitating C1q, C3a, and MAC blood concentrations in pregnant women can serve as an additional method to early identify FGR risks, disturbances in uteroplacental blood flow, and severe PE, e.g., C1q ≥ 250 ng/ml and MAC ≥ 2717 mAU/ml levels are associated with proper sensitivity and specificity for predicting adverse pregnancy outcomes.
► Including complement activation indicators in standard examination protocols will allow for personalized obstetric management, determining a need for hospitalization, choice of delivery method, and the intensity of fetal monitoring.
► The complement system can be considered as a new target for developing immunomodulatory and anti-complement drugs capable of limiting damage to trophoblast and endothelium.
Introduction. Preeclampsia (PE) remains one of the leading causes for maternal and perinatal morbidity and mortality. Placental insufficiency associated with impaired trophoblast invasion, hypoperfusion, and inflammatory endothelial activation is considered a key link to developing PE. In recent years, an interest to assessing a role of the complement system, an important innate immunity component involved in maintaining maternal-fetal tolerance has been growing. An imbalance in complement system activation may lead to damage to the trophoblast, altered placental blood flow, and development of pregnancy complications, including early-onset and late-onset PE as well as fetal growth restriction (FGR). Studying the activity of individual complement components (C1q, C3a, MAC) in PE allows to clarify the immune mechanisms underlying placental dysfunction and identify potential diagnostic and prognostic markers. However, the contribution of individual complement arms in severe PE remains poorly understood, thereby justifying clinically significance for investigating their levels and activity.
Aim: to determine diagnostic and prognostic value for complement system components (C1q, C3a and MAC) in pregnant women with severe PE, by taking into consideration differences between early-onset and late-onset disease forms to be compared with healthy pregnant women in control group.
Materials and Methods. A single-center observational study with cross-sectional comparative analysis at the inclusion stage and subsequent collection of perinatal outcomes was conducted among pregnant women with severe PE and healthy pregnant women with physiological pregnancy. There were enrolled 120 pregnant women, matched for age and gestational age, divided into 4 groups: with early-onset PE, developing at ≤ 34 weeks of pregnancy (n = 56); with late-onset PE, developing after 34 weeks (n = 32); control group 1 – healthy pregnant women with physiological pregnancy at ≤ 34 weeks (n = 17); control group 2 – healthy pregnant women with physiological pregnancy at > 34 weeks (n = 15). The analysis of clinical and laboratory parameters was carried out, which included demographic data, obstetric history, obstetric complications, concomitant diseases, hemostasis parameters, general clinical laboratory parameters, perinatal data, immunological parameters of the complement system – levels of C1q, C3a and membrane attack complex (MAC, C5b–C9). The levels of complement system components were quantitated by enzyme-linked immunoassay.
Results. In severe PE, complement system hyperactivation occurs, manifested by increased C1q, C3a and MAC levels. Complement component C1q concentrations ≥ 250 ng/ml were associated with developing FGR risk (p < 0.008). The C3a component was elevated in FGR and impaired uteroplacental blood flow, as well as in early-onset and late-onset PE. C3a values ≥ 615 ng/ml had moderate predictive ability for FGR (p = 0.004) and for blood flow disorders (p = 0.048). The terminal component of the complement system, MAC (C5b–C9) was significantly elevated in late-onset РЕ and FGR, indicating pathway activation and damage to trophoblast cells. A MAC cut-off value of ≥ 2717 mAU/ml predicted FGR development with sensitivity of 61.0 % and specificity of 82.0 % (p = 0.009).
Conclusion. The changes identified in our study confirm that excessive complement activation and MAC formation play a significant role in developing placental insufficiency, PE, and FGR, and that quantitating C1q, C3a, and MAC levels can be used as an additional biomarker tool for predicting pregnancy complications.

What is already known about this subject?
► Preeclampsia (PE) is a hypertensive disorder of pregnancy that increases risks for the mother and offspring in both the short and long term.
► PE is associated with an increased risk of maternal cardiovascular diseases later in life.
► Metabolic disorders increase the likelihood of both the development of PE and its long-term consequences.
What are the new findings?
► Women with PE were found to have lower parity and older age at delivery compared to control group.
► Previous PE is associated with persistent metabolic changes: higher body mass index and a significantly higher prevalence of grade II–III obesity years after labor.
► For the first time in the Russian population, it has been demonstrated that women with PE history who delivered female infants have a more than three-fold higher risk of hypertension in the future compared to patients whose pregnancies proceeded physiologically.
How might it impact on clinical practice in the foreseeable future?
► The results of the study confirm the need to develop personalized programs for the follow-up of women who have experienced PE.
► The importance of taking into account obstetric history (particularly PE) by therapists and cardiologists while assessing cardiovascular risk is emphasized.
► It is important to inform patients about PE long-term risks and to document this information in medical records to ensure continuity between specialists.
Introduction. Pregnancy and labor complicated by adverse conditions pose a threat not only to offspring but also to maternal health in later life. Preeclampsia (PE) has a long-term impact on maternal health, increasing the risk of subsequent somatic diseases. However, the number of studies investigating PE effects on maternal long-term somatic health are limited that determines the relevance of the present study.
Aim: to assess the somatic health of women with/without PE during pregnancy and labor who delivered female infants.
Materials and Methods. A retrospective case–control study was performed. A total of 1,302 medical records of women who delivered female infants in 2006–2007 were analyzed. The study sample included 198 patients meeting the inclusion criteria: spontaneous singleton gestation, term delivery of a live female infant in 2006–2007, and a medical record indicating either the presence or absence of PE. Based on obstetric history, the subjects were allocated to two groups: main group (n = 94), which included women diagnosed with PE during pregnancy and/or labor, and control group (n = 104), composed of women with uncomplicated pregnancies and labors. Archival obstetric records were analyzed, and somatic health was assessed based on medical documentation provided by the patients, including anthropometric measurements.
Results. The assessment of somatic health and anthropometric parameters revealed statistically significant differences between the study groups. Women with PE history showed a significantly higher prevalence of сardiovascular diseases, overweight, and obesity as well as lower parity compared with women whose pregnancies proceeded physiologically (p < 0.001). The probability of having hypertension was 3.297 times higher in PE group, with statistically significant difference (95 % confidence interval (CI) = 1.801–6.037; р < 0,001). No significant differences in the phenotypes of hypertension were identified. Notably, women with PE history were characterized by a significantly higher mean age of labor (p = 0.028), incidence of malignant neoplasms (p = 0.023) and a more frequently burdened family history of hypertension (p = 0.002). In addition, inter-group differences were considered statistically significant at p < 0.05.
Conclusion. Pregnancy complicated by PE increases the risk of subsequent cardiovascular diseases in general and hypertension in particular, overweight, and obesity in this group of patients. The data highlight the necessity for preconception prevention of hypertensive disorders, careful assessment of PE risk factors including family history and a personalized approach to the management of this patient cohort. These results underscore the importance of developing further strategies for PE prevention and early diagnosis, as well as implementing multidisciplinary long-term follow-up of women with PE history.
What is already known about this subject?
► Endometriosis of various locations causes infertility in 40 % of patients. The effectiveness of isolated drug therapy remains low.
► The degree of invasion of endometriosis foci is a determining factor in choosing an extent of surgical treatment.
► Radical surgical treatment of endometriosis in combination with drug therapy and assisted reproductive technologies increases the chances of pregnancy and its successful outcome.
What are the new findings?
► An inverse relationship between patients’ age and anti-Müllerian hormone level has been established.
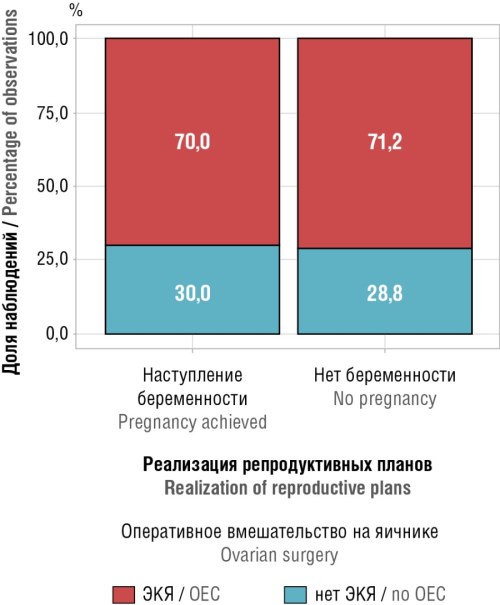
► Higher frequency of implemented patient reproductive plans was demonstrated while performing ovarian interventions due to ovarian endometriosis.
► The discriminatory ability of patient’s age in predicting ovarian endometriosis has been revealed.
How might it impact on clinical practice in the foreseeable future?
► The study results may contribute to increasing clinical treatment effectiveness for patients with endometriosis.
► An opportunity for predicting probability of age-related reproductive function in patients with endometriosis and the presence of ovarian endometriosis lesions is presented.
► Conducting comprehensive treatment of endometriosis (surgical and medical) will improve effectiveness of infertility treatment in this group of patients.
Aim: to determine the optimal tactics for managing patients with deep infiltrating endometriosis.
Materials and Methods. A prospective cohort clinical trial was conducted with 69 patients examined following surgical treatment for extensive infiltrating endometriosis and 3-month-long anti-relapse therapy with gonadotropin-releasing hormone agonists. Reproductive potential was assessed based on quantitating anti-Müllerian hormone (AMH) before and 6 months post-surgery, recording cases with/without onset of spontaneous pregnancy within 1 year.
Results. While comparatively analyzing AMH level in preand postoperative period revealed its decline in 51.8 % by average 0.152 ng/ml; the smallest reduction was found in women aged 28.5 to 33.5 years, regardless of the extent of surgical treatment. Pregnancy occurred in 10 of 43 planning women (average age 36,0 [32,0–42,5] years): 7 patients underwent ovarian interventions, 3 – surgical treatment for endometriosis of other localizations.
Conclusion. The data obtained evidence that subject’s age plays a decisive role in maintaining reproductive potential and a need for a differentiated approach in developing individual tactics for management and treatment of patients with deep infiltrating endometriosis, taking into account age, localization of endometriosis and reproductive plans.
What is already known about this subject?
► The data regarding lichen sclerosus (LS) onset and peak incidence in girls are unequal.
► The most common complaints of LS patients are presented as itching, dyspareunia and apareunia; the disease is often asymptomatic. The main LS clinical signs are described.
► There were compared the epidemiological features, clinical manifestations and concomitant autoimmune diseases in girls and adult women with LS. However, LS clinical features in girls of different age groups were not assessed.
What are the new findings?
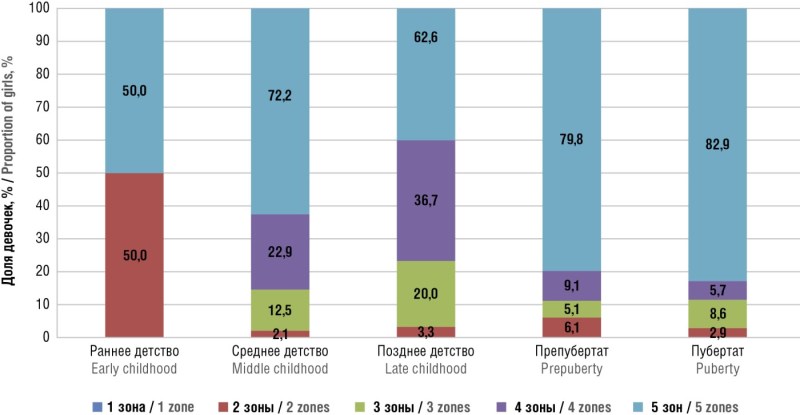
► LS is more often recorded in girls aged 5–6 years, at the transition from middle (3–5 years old)-to-late (6–8 years old) childhood.
► Asymptomatic LS is more common in younger age group (3–8 years old) girls.
How might it impact on clinical practice in the foreseeable future?
► Knowledge regarding LS incidence and its clinical features related to childhood age period may allow to correctly examine a pediatric patient, despite the lack of complaints to be diagnosed timely.
Aim: to study the features of lichen sclerosus (LS) clinically manifested in various age group girls.
Materials and Methods. A prospective observational study with 202 girls aged 0 to 18 years having verified LS clinical and histological diagnosis of LS was conducted. The age of LS onset was examined, determining the time from the appearance of the first symptoms to diagnosis was by analyzing most characteristic disease symptoms such as itching, changes in skin structure and color, the presence of cracks, constipation, dysuria, and lesion area related to childhood age period.
Results. It was found that 30 % LS girls noted the first disease symptoms at the age of 5–6 years (n = 67; 33.1 %). Among patients with vulvar LS, middle childhood (aged 3–5 years) girls predominated (n = 66, 32.7 %). Girls in early childhood (up to 2 years) and puberty period (13–17 years) were in minority comprising as few as 7 (3.5 %) and 19 (9.4 %) cases, respectively. The average LS duration before being properly diagnosed was 2.61 ± 0.13 years. In 27.7 % (n = 56) girls, the disease was asymptomatic, more often in younger patients aged 3–5 years (n = 10). Complaints of itching in the vulva, perineum and perianal area were reported in 58.9 % (n = 119) cases, but only five (2.48 %) girls had itching as a single complaint. In most cases, changes affected all 5 zones – the clitoris, labia minora, the inner surface of the labia majora, perineum and perianal area. A "figure eight"-like LS lesions of the genital tract were observed in 75.2 % (n = 152) girls, more often found in prepubertal (79.8 %; n = 79) and pubertal (82.9 %; n = 29) age.
Conclusion. LS incidence peaks during the transition from middle to late childhood. A more than nine-year observation was shown to shorten average duration of the disease before its diagnosis from 6 to 1.6 years. Analyzing pattern of complaints related to the age of girls allowed to conclude that LS exhibits no specific complaints, except for changes in vulvar skin structure and color, which are noticed only by 5 % patients. Itching in the vast majority of cases (n = 119; 58.9 %) is a consequence of arising complications such as cracks, ecchymosis and erosions.
What is already known about this subject?
► Preeclampsia (РЕ) remains one of the leading causes of maternal and perinatal morbidity and mortality, and most cases are still diagnosed at the stage of clinically manifest disease.
► Existing early prediction algorithms including the Fetal Medicine Foundation (FMF) approach and other combined models show high accuracy but often rely on costly biochemical biomarkers and standardized Doppler velocimetry, which limits their feasibility for large-scale screening, particularly in resource-constrained settings.
► Published machine learning models are frequently derived from relatively small, single-centre cohorts and rarely undergo independent external validation.
What are the new findings?
► This study presents a retrospective multiregional analysis based on routinely collected electronic health records (EНRs) data of pregnant women to predict РЕ risk at gestational age of ≤ 16 weeks.
► A multiparametric machine learning model (Extra Trees) was developed and evaluated using clinical, medical history and anthropometric predictors only, without biochemical biomarkers or Doppler indices, and underwent both internal and independent external validation.
► The model demonstrated robust discriminative performance (ROC-AUC around 0.86), high sensitivity and a very high negative predictive value at a clinically feasible risk threshold.
How might it impact on clinical practice in the foreseeable future?
► The proposed model can be embedded into clinical information systems and EНRs as an automated screening tool for early РЕ risk stratification requiring no additional laboratory or imaging tests.
► This may enable more rational routing of pregnant women to intensified surveillance and prophylaxis pathways (including aspirin prophylaxis and closer monitoring), particularly in resource-limited regions.
► Provided that local recalibration and prospective evaluation are undertaken, the model may support a shift from late РЕ detection towards proactive risk management in early pregnancy.
Introduction. Preeclampsia (PE) remains one of the leading causes of maternal and perinatal morbidity and mortality, while most cases are still diagnosed at the stage of clinically overt disease. Complex prediction algorithms incorporating biochemical biomarkers and Doppler velocimetry demonstrate high accuracy but are poorly suited for large-scale screening in resource-limited settings.
Aim: to develop, internally and externally validate mathematical models for predicting PE risk at gestational age of ≤ 16 weeks based on routine electronic health records (EНRs) data and machine learning methods.
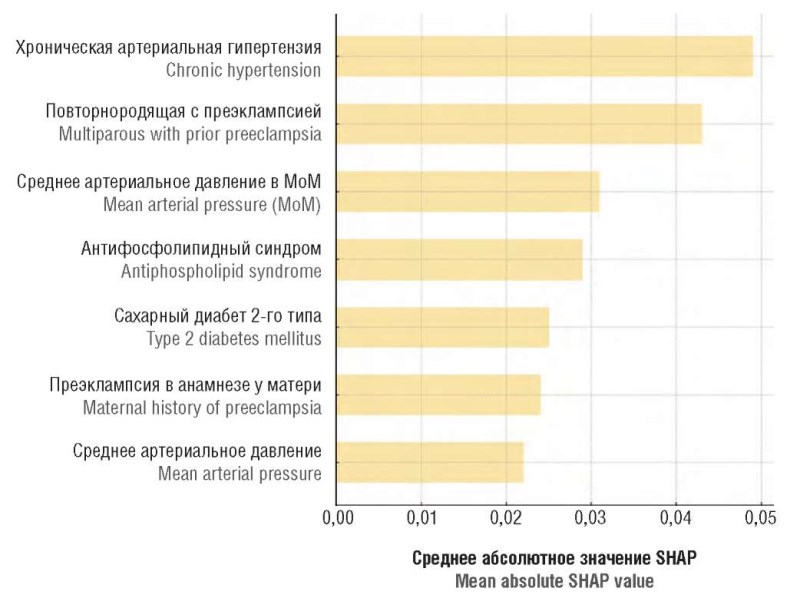
Materials and Methods. A retrospective cohort study was conducted using de-identified EНRs of pregnant women from eight regions of the Russian Federation spanning 2010–2025. The analytical dataset included 19,955 visits at gestational age ≤ 16 weeks. The composite outcome comprised PE, eclampsia and HELLP syndrome identified by ICD-10 codes. A broad spectrum of clinical, medical history and anthropometric variables was evaluated as potential predictors. Models (logistic regression, gradient boosting, Random Forest, Extra Trees) were trained with adjustment for class imbalance; feature selection was based on SHAP values (SHapley Additive exPlanations indices). Internal performance was assessed on a held-out test set, and independent external validation was performed on a subsample from healthcare facilities of the Republic of Karelia (n = 918).
Results. The final Extra Trees model including 35 clinically interpretable predictors achieved a ROC-AUC (Receiver Operating Characteristic curve; Area Under Curve) of 0.871 (95 % confidence interval (CI) = 0.811–0.923) and 0.862 (95 % CI = 0.833– 0.892) in internal and external validation set, respectively. At a probability threshold of 0.04, sensitivity in the external cohort was 0.886, specificity was 0.631, and negative predictive value (NPV) exceeded 0.99. Probability calibration was moderate (mean absolute calibration error was 0.245–24.5 percentage points). The strongest contributors to PE risk were chronic hypertension, history of PE, blood pressure parameters, antiphospholipid syndrome and diabetes mellitus.
Conclusion. The Extra Trees model developed on routinely collected EНRs data demonstrates acceptable discriminative ability, high sensitivity and very high NPV and may be considered as a screening tool for early PE risk stratification, provided local calibration assessment and further clinical evaluation.

What is already known about this subject?
► Pregnancy following in vitro fertilization (IVF) has a high risk of thrombotic and placenta-associated complications, which elevates manyfold upon onset of multiple pregnancies.
► Hemostasis is a key pathogenetic arm linking IVF, placenta-mediated pregnancy complications, thrombosis and adverse perinatal outcomes.
► The use of low molecular weight heparin (LMWH) at prophylactic doses in thrombotic risk groups requires no hemostasis monitoring.
What are the new findings?
► It has been shown that pregnancy progression in high thrombotic risk patients with multiple and induced pregnancies (post-IVF) is accompanied by hypercoagulation, and its correction as well as prevention of complications requires LMWH use at prophylactic doses often considered insufficient.
► Monitoring hemostasis parameters with dynamically checked thrombophilia markers during antithrombotic therapy allows for assessing the adequacy of anticoagulation and adjusting the dose of drugs to ensure effective and safe prevention of complications.
How might it impact on clinical practice in the foreseeable future?
► The data presented confirm the importance of monitoring hemostasis parameters during antithrombotic prophylaxis in risk groups (patients with burdened obstetric history and thrombophilia) while managing induced singleton and multiple pregnancies.
► Optimal anticoagulation assessed by measuring thrombophilia markers in dynamics, during early onset (at the stage of pregnancy planning/ovulation stimulation during IVF) allows to prevent thrombotic and effectively reduce gestational (preeclampsia, fetal growth restriction, etc.) complications including those with multiple gestations.
Aim: to evaluate the clinical significance of hemostasis control during anticoagulant therapy in patients with post-in vitro fertilization (IVF) pregnancy and burdened obstetric history (ВОН).
Materials and Methods. A prospective observational clinical comparative study was conducted. The main group consisted of 64 women with ВОН, with singleton (subgroup I1, n = 38) and multiple (dichoric diamniotic twins) pregnancies (subgroup I2, n = 26) following IVF, used low molecular weight heparins (LMWH). Control group: 35 pregnant women with singleton pregnancies (subgroup C1) and 35 with twins (subgroup C2) following IVF. Hemostasis was assessed by measuring APTT (activated partial thromboplastin time), PT (prothrombin time), TT (thrombin time), fibrinogen, antithrombin, protein C, protein S, protein C function (test РrоС Global); D-dimer; platelet aggregation with ristocetin, ADP (adenosine-5-diphosphate) and collagen, anti-Xa activity, thromboelastography, antiphospholipid antibodies and genetic thrombophilia.
Results. Post-IVF pregnancy in patients with ВОН and the risk of thrombosis during controlled anticoagulant prophylaxis was accompanied by lowered incidence of complications compared with control group: impaired uteroplacental blood flow was observed in 7.8 % vs. 24.3 % (p < 0.05), fetal growth restriction – in 3.1 % vs. 12.9 % (p < 0.05), preeclampsia – in 6.3 % vs. 20.0 % (p < 0.05), threat of pregnancy termination in the first trimester – in 14.1 % vs. 28.6 % (p < 0.05), in the second trimester – in 7.8 % vs. 21.4 % (p < 0.05). The controlled LMWH use was associated with favorable pregnancy course and outcome. Assessing dynamics of hemostasis parameters during anticoagulant and antiplatelet therapy allowed to substantiate the need to increase LMWH dose during pregnancy progression, to assess its adequacy and safety.
Conclusion. The increased hypercoagulation upon pregnancy progression requires monitoring the adequacy of anticoagulation therapy in risk groups, especially in post-IVF multiple pregnancies.
REVIEW ARTICLES
What is already known about this subject?
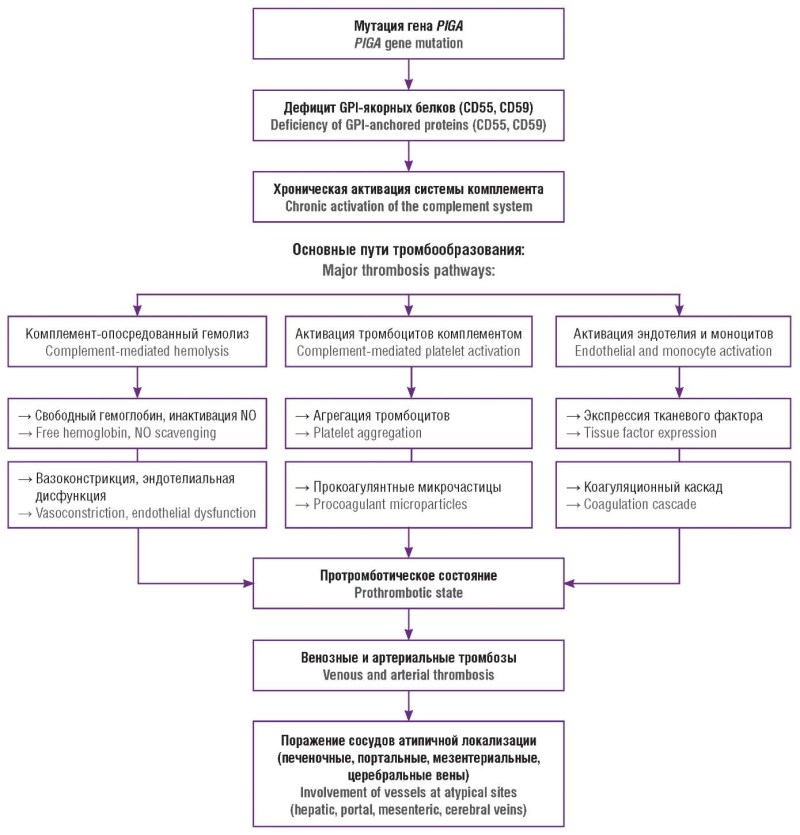
► Paroxysmal nocturnal hemoglobinuria (PNH) is associated with a high risk of venous thrombosis, often leading to atypical vascular sites and determining patient prognosis and mortality.
► Deficiency of GPI-anchored complement regulatory proteins results in uncontrolled complement activation, linking intravascular hemolysis with endothelial dysfunction and PNH thrombotic complications.
► Pregnancy and postpartum period represent states of heightened complement activation and hypercoagulability, substantially increasing the risk of hemolytic and thrombotic events in women with PNH.
What are the new findings?
► Current concepts of thrombosis pathogenesis in PNH have been systematized, emphasizing the interplay between complement activation, endothelial dysfunction, nitric oxide depletion, and subsequent activation of the coagulation cascade.
► The clinicopathogenetic continuum between PNH, aplastic anemia, and myelodysplastic syndromes in the context of immune damage to the bone marrow is analyzed.
► Contemporary multidisciplinary strategies for pregnancy management in PNH in the era of complement-inhibitory the-
rapy are summarized.
How might it impact on clinical practice in the foreseeable future?
► Increasing awareness of PNH in patients with unexplained thromboses and cytopenias may facilitate earlier diagnosis and timely initiation of pathogenetic therapy.
► Interdisciplinary management of reproductive-age patients with PNH may reduce maternal and perinatal risks.
► Wider implementation of complement inhibition is expected to modify the natural history of PNH by reducing thrombotic burden, and disease-related mortality.
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare acquired clonal hematopoiesis disorder caused by a somatic mutation in the PIGA (phosphatidylinositol glycan, class A) gene, resulting in deficiency of glycosylphosphatidylinositol (GPI)anchored complement regulatory proteins on blood cell surface. Dysregulation of the complement system leads to chronic intravascular hemolysis, anemia, endothelial dysfunction as well as development of prominent acquired thrombophilic state, clinically manifested by venous thromboembolism, frequently involving atypical vascular sites. Thrombotic complications represent the leading cause of adverse outcomes and mortality in patients with PNH. This review summarizes current evidence on PNH etiology, molecular genetics and pathophysiological mechanisms including complement dysregulation, nitric oxide depletion, intraand extravascular hemolysis, and the multifactorial pathogenesis of thrombosis. The clinicopathogenetic relationship between PNH, aplastic anemia, and myelodysplastic syndromes is discussed in the context of immune-mediated bone marrow failure. Special emphasis is put on PNH course in women of reproductive age. Physiological changes associated with pregnancy and the postpartum period, including complement activation and hypercoagulability, are shown to be associated with increased risk of hemolytic crises and thromboembolic complications in women with PNH, thereby defining the disease as a condition of extremely high obstetric risk. Contemporary principles for multidisciplinary management aimed at improving maternal and perinatal outcomes are reviewed.
What is already known about this subject?
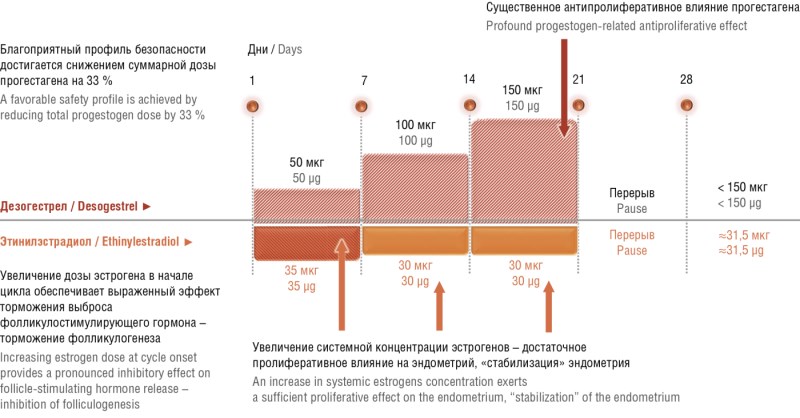
► Three-phase combined oral contraceptive (СОС) containing ethinyl estradiol and desogestrel (EE/DSG) is a highly effective low-dose combined contraceptive.
► Few adverse events have been reported upon using three-phase EE/DSG-based COC.
► Three-phase EE/DSG-based exerts additional positive effect by improving skin condition, associated with weakening of the androgenic effect.
What are the new findings?
► Clinical situations coupled to priority choice of a three-phase EE/DSG-based COC are systematized, with new data on cycle control related to it are presented.
► For the first time, a review with references to relevant studies presents information on the lack of influence of a three-phase COC with EE/DSG on myomatous nodes with a diameter of up to 22 mm in comparison with monophasic СОС.
► For the first time, the review citing relevant studies presents information on improving the quality of life upon using a three-phase EE/DSG-based COC in women with uterine fibroids without indications for surgical treatment.
How might it impact on clinical practice in the foreseeable future?
► Optimizing patient contraception counseling.
► Improving personalized choice of COCs in various clinical situations.
This article presents general information on demographic processes in Russia and the relevance of using highly effective contraception methods particularly combined oral contraceptives (COCs), to prevent artificial abortions. The importance of high-quality counseling for prescribing estrogen-progestogen medications is emphasized. Clinical situations for the preferential choice of a three-phase combined ethinyl estradioland desogestrel-based contraceptive are described.
What is already known about this subject?
► There is evidence about increased cord blood levels of brain natriuretic peptide (BNP) in neonates with fetal growth restriction, indicating its potential role in assessing fetal well-being.
► In obstetrics, BNP has been studied in various conditions such as gestational hypertension and preeclampsia, as well as in case of fetal distress and cardiovascular disease.
► In neonates, BNP level may serve as an indicator of cardiovascular diseases and be used to monitor response to treatment.
What are the new findings?
► The relevance of using BNP not only in cardiology, but also in obstetrics and neonatology is emphasized.
► Assessing BNP level is useful in neonates in intensive care units and for diagnostics of congenital heart defects and other serious conditions such as bronchopulmonary dysplasia and persistent pulmonary hypertension.
► The effectiveness of measuring BNP level as an adjunct to echocardiography in assessing myocardial function in infants has been confirmed, which may markedly improve diagnosis and treatment.
How might it impact on clinical practice in the foreseeable future?
► The introduction of BNP testing into clinical practice may substantially change the approach to diagnosing and monitoring cardiovascular diseases in newborns and pregnant women.
► Using BNP biomarker may allow doctors to assess patients more quickly and accurately, which could lead to more timely interventions and improved treatment outcomes. In particular, it may improve the diagnostics of congenital heart defects and other conditions that require emergency care.
► Integration of BNP into clinical protocols may facilitate a more individualized approach to treatment and improve patient monitoring in intensive care units.
Brain natriuretic peptide (BNP) is a well-known marker in cardiology used for the diagnosis, prognostic assessment, and treatment selection in patients with congestive heart failure. In obstetrics, BNP has been studied in pregnant women with gestational hypertension, preeclampsia, fetal distress, cardiovascular diseases, and gestational diabetes mellitus. Elevated BNP levels have been reported in the umbilical blood of newborns with intrauterine growth restriction. Recent studies indicate that BNP is also useful in assessing newborns condition and predicting neonatal adaptation. In children, BNP serves as an indicator of heart diseases and can be used to monitor treatment response. The diagnostic role of plasma BNP in newborns admitted to intensive care units has shown promise as an auxiliary marker in diagnosing congenital heart defects, bronchopulmonary dysplasia, patent ductus arteriosus, and persistent pulmonary hypertension, as well as in acute heart failure. Most studies evaluating cardiac dysfunction and myocardial injury in newborns rely on echocardiography; however, myocardial function can also be assessed using plasma biomarkers. BNP has proven to be an invaluable complement to echocardiography in evaluating ventricular function in infants and children.
What is already known about this subject?
► Amniotic fluid embolism (AFE) was considered a mechanical obstruction of pulmonary vessels by amniotic fluid elements, identified in animal experiments and clinical observations.
► Traditionally, AFE is characterized by the sudden development of critical hypoxia, severe arterial hypotension, and severe coagulopathy (DIC) during or immediately after labor.
► AFE remains one of the most dangerous causes of maternal mortality, characterized by a fulminant course and difficulty in early diagnosis.
What are the new findings?
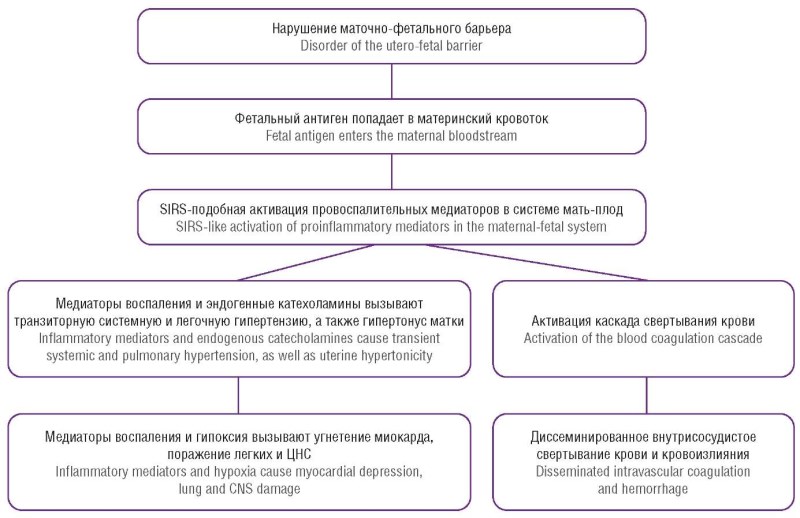
► The shift from the term "embolism" to "anaphylactoid syndrome of pregnancy" (ASP) is justified, because systemic response to inflammatory mediators rather than mechanical obstruction plays a key role.
► Similarities between the ASP pathogenesis and septic and anaphylactic shock have been established, where the cascade of reactions is triggered by vasoactive mediators: histamine, bradykinin, and cytokines.
► Monoclonal antibodies have been proposed as specific pathological markers for diagnostics, allowing for the detection of fetal elements in microvessels.
How might it impact on clinical practice in the foreseeable future?
► Identification of risk groups: increased attention should be paid to risk groups to enhance vigilance.
► The introduction of modern laboratory tests (assessing antithrombin III, D-dimer) will ensure a more rapid transition from a "diagnosis of exclusion" to pathogenetically justified ASP confirmation.
► The focus will shift to preventing precipitating factors such as unnecessary oxytocin stimulation and early mediator therapy (e.g., leukotriene inhibitors).
Amniotic fluid embolism (AFE) is a rare, life-threatening obstetric complication, known in modern terminology as anaphylactoid syndrome of pregnancy (ASP). ASP is an acute reaction triggered by the penetration of amniotic fluid (containing fetal cells, meconium, tissue factor, etc.) into the maternal circulatory system. This leads to a cascade of pathological reactions comprising the classic triad of fetal hypoxia: acute hypoxia (dyspnea, cyanosis), circulatory collapse (shock, cardiac arrest), and coagulopathy (bleeding). Fetal hypoxia is a diagnosis of exclusion; its treatment is aimed at combating the three main threats: respiratory failure, hemodynamic collapse, and coagulopathy. The prognosis is extremely grave, with maternal mortality reaching 80–90 %. Perinatal mortality and morbidity are also very high due to acute fetal hypoxia. ASP remains one of the most dangerous and poorly predicted causes of maternal mortality. A high level of physician vigilance, awareness of early symptoms, and immediate initiation of comprehensive resuscitation and intensive care aimed at maintaining oxygenation, hemodynamics, and correcting coagulopathy are crucial. The modern therapeutic approach to the syndrome as an anaphylactoid reaction justifies the use of high glucocorticosteroid doses.
What is already known about this subject?
► Human papillomavirus (HPV) is a major risk factor for developing cervical cancer (CC).
► The main laboratory and diagnostic methods for СС screening currently consist of cytological examination of cervical scraping as well as HPV testing for cancer risk in addition to cytological cervical screening.
What are the new findings?
► The article describes contemporary methods and diagnostic tests for HPV infections and HPV-associated diseases, the relevant results following medical specialist interpretation, as well as rare forms of carcinomas, additionally discusses data variability.
How might it impact on clinical practice in the foreseeable future?
► The availability of test assays continue to increase rapidly, and in the near future, the features and nuances of research data may be increasingly discussed, allowing to identify the most controversial issues and relevant solutions as well as expand the new research planning horizon.
Human papillomavirus (HPV) is the main risk factor for developing cervical cancer (CC). About 70–75 % of all invasive CC cases worldwide are associated with HPV 16 and 18 genotypes, 20–25 % cases being related to HPV 31, 33, 35, 45, 52, and 58 genotypes. Currently, there are more than 100 tests for HPV diagnostics, but up to now, it has been difficult to establish and evaluate sensitivity of cytological examination for detecting pre-invasive and invasive cervical squamous and glandular lesions. The use of biomarkers for a more objective diagnostics of squamous intraepithelial lesions (SIL) was investigated in numerous studies. The most widely used biomarker is the p16INK4a (p16) antibody that flags E7-induced high-risk HPV-caused cell proliferation. The diagnosis of SIL upon cervical biopsy is also highly variable convincingly supported by the documented evidence. The intermediate category, cervical intraepithelial neoplasia grade 2 (CIN2), provides the least reproducible results. The use of immunohistochemistry p16, alone or in combination with the proliferation marker Ki-67, increases the effectiveness of differentiation between SIL and its benign imitators. Thus, a high degree of variability still is observed between the data of cervical cytology and biopsy due to both sampling errors and the expertise of medical works involved in data interpretation. Atypical squamous cells of undetermined significance (ASC-US) represent the primary source of such variability.

What is already known about this subject?
► In women of advanced reproductive age, a decline in ovarian reserve is a natural age-related process accompanied by a reduction in both the number and quality of follicles, which markedly decreases the likelihood of spontaneous conception and increases the risk of pregnancy loss.
► Ovarian reserve deficiency is associated with hormonal imbalance – reduced anti-Müllerian hormone (AMH), elevated follicle-stimulating hormone, ovulatory dysfunction, and altered endometrial receptivity, resulting in obstacle in implantation and reduced effectiveness of assisted reproductive technologies (ART).
► Current diagnostic methods including assessing AMH level, antral follicles count (AFC), as well as genetic and immunological markers together with innovative approaches such as PRP therapy (platelet-rich plasma therapy), growth factors, and cellular technologies, demonstrate promising potential in fertility restoration. However, their clinical efficacy and long-term safety analysis require further investigation.
What are the new findings?
► The application of innovative methods (PRP therapy, growth factors, and cell-based technologies) opens up new avenues for restoring ovarian function in women of advanced reproductive age by improving ovarian blood supply and stimulating follicular growth.
► Development of personalized protocols for controlled ovarian stimulation taking into account AMH level, AFC, and genetic markers, enhances the efficiency of retrieving high-quality oocytes and improves ART outcomes.
► The integration of traditional hormonal therapy with advanced biotechnologies and supportive measures (antioxidants, mitochondrial therapy) provides a comprehensive approach that increases the chances for successful conception and pregnancy maintenance.
How might it impact on clinical practice in the foreseeable future?
► The implementation of individualized ovarian stimulation protocols, taking into account age, AMH level, and AFC, will enable physicians to tailor treatment more precisely in women of advanced reproductive age with diminished ovarian reserve, thereby increasing the chances for successful conception.
► The use of innovative approaches (PRP therapy, stem cells, mitochondrial support) may markedly improve the quality of oocytes and embryos, minimizing a risk of complications and enhancing effectiveness of ART programs.
► Optimizing diagnostic and therapeutic algorithms will reduce the timeframe required to achieve pregnancy, decrease the costs associated with multiple in vitro fertilization attempts, and improve treatment safety for patients.
Aim: to systematize current data on diagnostic potential and therapeutic approaches to restore fertility in women of advanced reproductive age with diminished ovarian reserve, as well as to identify promising directions for further research.
Materials and Methods. The review includes scientific publications indexed in PubMed/MEDLINE, Scopus, Web of Science, Google Scholar spanning from January 2020 to January 2025 inclusive, according to the indexing status at the time of the literature search. Article selection was performed in accordance with the PRISMA international guidelines. At the initial search stage, 397 publications were identified in PubMed/MEDLINE, 96 in Scopus, 121 in Web of Science, and 28 in Google Scholar. Duplicate and non–full-text records were excluded. After the selection procedure, 60 publications were included in the final review, comprising randomized clinical trials, meta-analyses, systematic reviews.
Results. Literature analysis demonstrated that the assessment of anti-Müllerian hormone levels and the antral follicle count remain the most reliable predictors of ovarian reserve and treatment outcomes. Individualized protocols for controlled ovarian stimulation improve the rate of mature oocyte retrieval; however, their efficacy is limited by age-related decline in oocyte quality. Experimental approaches such as platelet-rich plasma (PRP) therapy, stem cell application, and mitochondrial support show promising results in pilot studies but require further standardization and evaluation of long-term safety. The use of donor oocytes remains the most effective strategy in cases of severe ovarian reserve depletion.
Conclusion. Despite advances in elucidating the pathogenesis of ovarian aging, optimizing fertility restoration in women of advanced reproductive age with diminished ovarian reserve remains a multifactorial challenge. The most promising directions include the individualized selection of stimulation protocols, integration of supportive and experimental methods, as well as development of molecular and genetic biomarkers for personalized therapy.
CLINICAL CASE

What is already known about this subject?
► Placenta accreta spectrum (PAS) disorders are strongly associated with prior cesarean delivery and placenta previa, with incidence rising in parallel with increasing cesarean section rates.
► Ultrasound, especially with color Doppler, is the primary imaging modality for antenatal PAS diagnosis; however, differentiating between placenta accreta, increta, and percreta remains challenging.
► Magnetic resonance imaging (MRI) serves as a complementary tool in complex or inconclusive cases, particularly in posterior placenta or suspected deep invasion into adjacent organs.
What are the new findings?
► Early identification of the “rail sign” on color Doppler provided an initial marker of placenta increta, later confirmed by MRI and histopathology.
► Serial ultrasound monitoring from 8 to 28+6 weeks of gestation documented the progression of placental invasion, offering practical guidance for clinicians managing high-risk pregnancies.
► The integration of Doppler markers with MRI findings reinforced diagnostic accuracy, demonstrating their combined value in planning delivery strategies and improving maternal outcomes.
How might it impact on clinical practice in the foreseeable future?
► Routine incorporation of Doppler markers, such as the “rail sign,” into PAS screening may allow earlier and more reliable detection of abnormal placentation.
► Serial ultrasound monitoring protocols could improve risk stratification, guide delivery planning, and reduce emergency interventions in high-risk pregnancies.
► Combining ultrasound and MRI findings may establish a more standardized diagnostic route, optimizing surgical preparedness and improving maternal-fetal outcomes.
Introduction. The rising global incidence of cesarean deliveries has led to elevated abnormal placentation, particularly placenta accreta spectrum (PAS) disorders. These conditions represent serious obstetric complications with high risks for both maternal and fetal morbidity and mortality.
Аim: to analyze a clinical case of placenta increta with deep invasion, highlighting the diagnostic value of advanced ultrasonographic techniques.
Case presentation. A 29-year-old pregnant woman with a history of three cesarean sections (2014, 2017, and 2025) and prominent somatic comorbidities (chronic pyelonephritis and urolithiasis) underwent routine antenatal ultrasound screenings at 8, 12, 20, 23, and 28+6 weeks of gestation. Standard transvaginal and transabdominal sonographic techniques were used. After sonographic suspicion of placenta increta, magnetic resonance imaging (MRI) was performed for verification. Final diagnosis was confirmed intraoperatively and through histopathological analysis. Ultrasound revealed signs consistent with PAS type 2 (placenta increta): marked thinning of the myometrium, dilated lacunae, retroplacental hypervascularization, and placental bulging. At 28+6 weeks, transvaginal sonography detected further invasion into the cervical canal (PAS 3a). Color Doppler imaging revealed vascular "rail signs," indicating deep invasion. MRI confirmed complete placenta previa with abnormal tissue growth into the uterine scar and myometrial layers. This case demonstrates the effectiveness of modern ultrasonography and Doppler imaging in the early identification and classification of PAS disorders. Although previous publications emphasized limitations in determining invasion depth via ultrasound, this report highlights its diagnostic reliability, especially when complemented by MRI. Early diagnosis is essential for surgical planning and improving perinatal outcomes.
Conclusion. Ultrasound primarily combined with color Doppler imaging, provides a reliable and non-invasive means for diagnosing PAS disorders. In this case, the identification of specific Doppler features – particularly the "rail sign" representing vascular bridging between the myometrium and serosa – proved critical for diagnosing placenta increta. These findings highlight a potential for advanced Doppler markers in improving antenatal detection and surgical planning. Integrating such diagnostic techniques into routine care can markedly improve maternal and fetal outcomes in high-risk pregnancies.
RETRACTION NOTE
The following article is retracted: Policheva A.A., Oganesyan E.A., Yarushkina I.S., Martynenko A.S., Kormukhina E.E., Taimova Ch.O., Mustafina A.R., Kim V.V., Valitova A.A., Suleimanov N.R., Gaibaryan K.A., Radzhabov M.E., Baimukhambetova A.E., Razumova A.E. The role of sphingolipid metabolism in female reproductive health disorders. Akusherstvo, Ginekologia i Reprodukcia = Obstetrics, Gynecology and Reproduction. 2025;[published online]. (In Russ.). https://doi.org/10.17749/2313-7347/ob.gyn.rep.2025.691. An unattributed translation (i.e. plagiarism) has led to the retraction.
Events
2026-03-23
Take a survey for healthcare professionals on the use of artificial intelligence in healthcare
Survey: The use of AI technologies in medical activities
Direct hyperlink: https://anketolog.ru/rs/1013120/Ea6s6qUk
QR-code:

| More Events... |

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
ISSN 2500-3194 (Online)






































