


“Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) is a scientific and practical peer-reviewed journal for obstetricians, gynecologists and other experts in the area of women’s health. Our aims and priorities focus on scientific and information support to the members of the "professional community" in their pursuit of new ideas in obstetrics and gynecology research. In addition, the AGR journal proudly contributes to the continuing medical education (CME) of practitioners who specialize in various areas of women’s health including obstetrics, gynecology, in vitro fertilization (IVF) and assisted reproductive technology (ART).
“Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) was founded in 2007
The impact factor of this journal, as shown in the Russian Science Citation Index (RSCI) is among the highest for the periodicals on obstetrics, gynecology, perinatology and problems of women’s health. According to RSCI, the biennial impact factor was 0.509 in 2013, 0.810 in 2014, and 0.976 in 2015.
The journal publishes original articles on clinical and experimental studies, as well as reviews on obstetrics, gynecology, and human reproduction. Special attention is paid to publications on CME as well as historic aspects of obstetrics and gynecology. All manuscripts, both original research and literature reviews, are published upon a mandatory peer-review.
Languages: Russian, English
Periodicity: 6 issues per year.
The printed versions are distributed under the Creative Commons Attribution 4.0 License: full-text materials are freely available to the public in an open access repository.
Distribution of the printed version: Russia, the EurAsian Economic Community (EurAsEC) countries (Belarus, Kazakhstan, Kyrgyzstan, Tajikistan, Uzbekistan, Armenia, Moldova), Ukraine, Georgia.
The editorial board of “Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) includes leading scientists from Russia, Austria, Great Britain, Israel, USA, Croatia, Ukraine, Georgia, and Uzbekistan.
The editorial board of this journal maintains the policy of full compliance with all principles of publishing ethics. Our ethical standards and codes conform to those of top international science publishers.
All submitted materials undergo a mandatory double-blind peer review.
Media Certificate of Registration: ПИ №FS77-34885 of December 29, 2008.
ISSN 2077-8333 (Print)
ISSN 2311-4088 (Online)
By the decision of the Higher Attestation Commission (HAC) of Russia, “Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) is included in the "List of top peer-reviewed scientific journals and publications" where scientists seeking academic degrees are required to publish their results.
The “Obstetrics, Gynecology and Reproduction” (“Akuserstvo, Ginekologia i Reprodukcia”) journal appears in the Russian Universal Scientific Electronic Library (RUNEB) elibrary.ru and is also present in the database of the Russian Science Citation Index (RSCI). Concise versions of major articles from this journal are published by the All-Russian Institute for Scientific and Technical Information (VINITI). The journal is also indexed by "Ulrich's periodicals Directory" – a global information system of periodicals and continued publications.
Current issue
EDITORIAL
The editorial article is devoted to the key scientific and clinical directions presented in the journal’s second issue for 2026. The articles in this issue are focused on the analysis of pathogenetic mechanisms that determine the course of pregnancy, the development of obstetric and gynecological diseases, reproductive prognosis, and long-term clinical outcomes. Particular importance is given to studies addressing preeclampsia, placental and endothelial dysfunction, immune regulation, complement system abnormalities, venous thromboembolism, fertility preservation, estrogen-dependent proliferative diseases, and endocrine disorders during pregnancy. The materials of this issue reflect the current trend toward an integrative analysis of pathogenesis, in which obstetrics and gynecology are considered in close connection with immunology, endocrinology, angiology, gynecologic oncology, and reproductive medicine. This approach emphasizes the importance of early diagnosis, personalized treatment strategies, assessment of long-term disease consequences, and preservation of patients’ quality of life.
ОRIGINAL ARTICLES
What is already known about this subject?
► Preeclampsia (PE) is a multifactorial, multisystemic complex syndrome that occurs due to abnormal pregnancy, with underlying pathogenesis involving the release of iron hormones and ferroptosis.
What are the new findings?
► The study results not iron deficiency, but rather a completely different role for iron metabolism markers in PE pathogenesis evidenced by significantly increased ferritin levels in both early- and late-onset PE.
► Soluble transferrin receptors like latent iron-binding capacity of blood serum are an informative marker of iron deficiency. However, in PE, a paradoxical rise in receptor levels is observed potentially due to destruction of high-level-transferrin receptor-positive trophoblast cells during placental ischemia and oxidative stress.
► The difference among these parameters peaked in pregnant women with fetal growth restriction (FGR), with soluble transferrin receptors exceeding by 26.7 % that of in PE without FGR being most informative parameter.
How might it impact on clinical practice in the foreseeable future?
► Progress in understanding complex PE pathogenesis and revisiting both its diagnostic and prognostic markers, which may help in risk stratification of both early and late PE, cautions to widely use iron supplements and emphasizes the need for a personalized treatment approach.
► It is recommended to include in the patients management algorithm assessing concentration of ferritin, serum iron, transferrin, haptoglobin, hepcidin 25 and the level of soluble transferrin receptors in the second trimester of pregnancy to identify women susceptible to developing PE and FGR.
Aim: to determine iron metabolism parameters in the blood of pregnant women with different preeclampsia (РЕ) phenotypes.
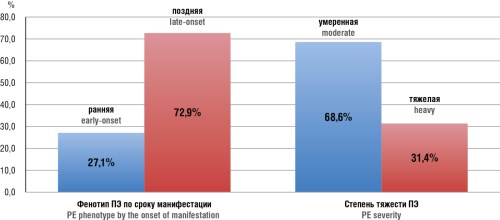
Materials and Methods. A single-center prospective comparative case-control study was conducted that assessed clinical, anamnestic, laboratory, and instrumental data of 95 pregnant women, divided into two groups: the main group (70 pregnant women with diagnosed early- and late-onset PE) and control group (25 women of similar age without significant extragenital and gynecological pathology, without PE) with a favorable outcome of pregnancy and childbirth. The analysis was conducted in main group depending on PE manifestation. It was found that in main group 19/70 (27.1 %) pregnant women were with early-onset PE; 16/19 (84.2 %) of them had severe PE with fetal growth restriction (FGR), the remaining 3/19 (15.8 %) women had moderate PE without FGR. Late PE manifestation was observed in 51/70 (72.9 %) pregnant women; 6/51 (11.8 %) had severe PE with FGR, 45/51 (88.2 %) had moderate PE. In late-onset PE, one FGR case was identified at 35+5 weeks of gestation. In main group, 23 (32.9 %) observations with PE and FGR were found. Iron metabolism parameters (hemoglobin level and erythrocyte characteristics, serum iron content, transferrin, ferritin, latent iron-binding capacity of blood serum, haptoglobin, soluble transferrin receptors and hepcidin 25) were studied thoroughly in patients with earlyand late-onset PE.
Results. The ambiguity and divergence of iron metabolism parameters in developing early- and late-onset PE were demonstrated. Among women with subsequent manifestation of both early- and late-onset PE at the onset of the second trimester of pregnancy, 8/70 (11.4 %) patients received iron therapy. Our results indicate not detected iron deficiency, but rather a completely different value for iron metabolism markers in PE pathogenesis. In particular, in early-onset PE, the ferritin level was 3.46 times higher than that of in the second trimester of uncomplicated pregnancy, whereas in late-onset PE, it was 5.78 times higher than in the third trimester in control group. In early-onset PE, the level of transferrin receptors was 1.78 mg/L vs. 0.75 mg/L in women with uncomplicated pregnancy at the same time, which is 2.37 times higher. In late-onset PE, the level of receptors was 1.93 mg/L, which is 1.72 times higher than in the third trimester of uncomplicated pregnancy. The haptoglobin level in early-onset PE was 102.4 mg/dL vs. 65.5 mg/L in the second trimester of uncomplicated pregnancy, which is 1.56 times higher. In late-onset pregnancy, the haptoglobin level was 134.5 mg/dL vs. 46.3 mg/dL in the third trimester of uncomplicated pregnancy, which is 2.9 times higher. The difference in iron metabolism parameters in pregnant women with FGR vs. uncomplicated pregnancy peaked, with level of soluble transferrin receptors, which amounted to 2.09 mg/L and was 26.7 % higher than in PE without FGR most informative.
Conclusion. PЕ is associated with iron imbalance, characterized by maternal iron overload and relative fetal iron deficiency due to placental dysfunction. It cautions to widely use iron supplements and emphasizes the need for a personalized treatment approach. Thus, our findings contribute to our understanding multifaceted PE pathogenesis and revisiting both its diagnostic and prognostic markers, which may aid in risk stratification for early-onset and late-onset PE.
What is already known about this subject?
► Bariatric surgery, particularly laparoscopic sleeve gastrectomy (LSG), is highly effective for obesity treatment, reducing body mass index (BMI) by over 14 kg/m2 within 12 months.
► Patients subjectively link post-bariatric weight loss to improved fertility, yet reported pregnancy rates vary widely (22–92 %).
► Currently, the key pregnancy predictor is the post-operative BMI achieved: BMI reduction by > 5 kg/m2 is significantly associated with successful conception, increasing its chances by 20.2-fold.
What are the new findings?
► A significant postoperative decline in anti-Müllerian hormone (AMH) and antral follicle count (AFC) is a novel negative post-LSG pregnancy predictor emphasizing a role for ovarian reserve dynamics beyond achieved BMI.
► Patient’s profile at high infertility risk post-surgery has been identified: smoking, a family history of early or premature menopause, and a history of ovarian surgery.
► It was found that patients with higher baseline BMI and insulin resistance achieved pregnancy post-surgery more often using assisted reproductive technologies, despite greater absolute weight loss.
How might it impact on clinical practice in the foreseeable future?
► The results obtained justify a need for applying a predictive approach: pre-LSG assessment of insulin resistance, ovarian reserve, and reproductive history enables personalized fertility prognosis and treatment planning for each patient.
Aim: to evaluate an effect of laparoscopic sleeve gastrectomy (LSG) on fertility in obese reproductive age women and to identify factors associated with subsequent pregnancy.
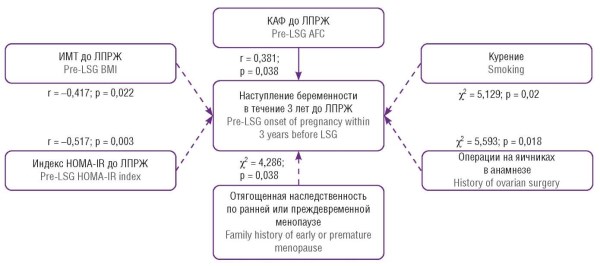
Materials and Methods. This single-center observational retrospective comparative study included 48 women aged 25–36 years who underwent LSG. Body mass index (BMI), insulin resistance index HOMA-IR (Homeostasis Model Assessment of Insulin Resistance), anti-Müllerian hormone (AMH), and antral follicle count (AFC) were assessed before and 12 months post-surgery. Smoking history, family history of premature menopause, and prior ovarian surgery were analyzed. After 3 years post-surgery, patients planning pregnancy were stratified as follows: Group 1 – achieved pregnancy (n = 16, including 10 spontaneous and 6 through assisted reproductive technologies), Group 2 – no pregnancy (n = 14).
Results. Following LSG, significant reductions were observed in BMI (from 44.2 to 31.3 kg/m2; p = 0.001) and HOMA-IR index (from 8.3 to 5.1; p = 0.001). Pregnancy occurred in 53.3 % of patients. Women who did not conceive had higher baseline BMI (47.1 kg/m2 vs. 41.5 kg/m2; p = 0.025), HOMA-IR index (10.2 vs. 5.8; p = 0.005), and more pronounced decline in ovarian reserve post-LSG: AMG level was 0.89 vs. 2.65 ng/ml (p = 0.001). Significant risk factors included familial history of premature menopause (85.7 %), ovarian surgery (42.9 %), and smoking (78.6 %). Correlation analysis revealed significant negative associations between pregnancy likelihood and baseline BMI (r = –0.42; p = 0.02) and HOMA-IR (r = –0.52; p = 0.003), whereas AFC showed positive correlation (r = 0.38; p = 0.04). Statistically significant associations were found between pregnancy and smoking (p = 0.02), prior ovarian surgery (p = 0.02), and familial history of early menopause (p = 0.04).
Conclusion. LSG use was associated with improved metabolic parameters and fertility recovery in 53.3 % of patients. However, given the small sample size, these findings require validation in larger-scale cohorts. The likelihood of achieving pregnancy depends on a complex interplay between the examined factors, underscoring a need for individualized risk assessment and a personalized approach to therapy.
Highlights
What is already known about this subject?
► Preterm delivery is associated with high incidence of neonatal cerebral morbidity especially cerebral palsy and encephalopathy.
► Antenatal magnesium sulfate (MgSO4) infusion had been used for neuroprotection for preterm baby, with significant effectiveness.
► There are different protocols for MgSO4 infusion during pregnancy with different dosages, with non-global agreement for the dose or the duration.
What are the new findings?
► There was no difference between all regimen in the effect of neuroprotection.
► The least dose and least duration had the same effect as the larger dose and larger duration.
► Use the least dose and duration (loading dose 4 g over 30 minutes) can protect the female form the side effect of the drug with the same neurprotcetive effect for the baby.
How might it impact on clinical practice in the foreseeable future?
► The use of the smallest dose with shorter duration of MgSO4 (loading dose 4 g over 30 minutes) for neuroprotection is proved and could be generalized, and it could significantly decrease the morbidity and mortality of preterm neonates.
Aim: to assess the comparative effectiveness and adverse effects of different magnesium sulfate (MgSO4) regimens for fetus neuroprotection in women who are considered at risk of preterm birth.
Materials and Methods. This randomized controlled clinical single-center study was taken place at the Obstetrics and Gynecology Department of Tanta University Hospital, a tertiary care referral center and neonatology department. The research was carried on pregnant female with gestational age 24–34 weeks with established preterm labor. The patients were sorted into four groups at random. Number of cases in each group was 20 cases, and they were assigned to one of the four groups using a computer-based program. All groups of women had received care in accordance with accepted clinical standards. Throughout the infusion, the protocol required that the mother's heart rate, blood pressure, breathing rate, tendon reflexes, and any negative effects be recorded. Throughout labor, the fetal heart rate had been checked. Mothers and their newborns were monitored until they were released from the hospital.
Results. There are different regimens for its use, and there was no difference between all the regimens in its effect for neuroprotection either clinically or radiologically or in its safety, so we recommend the use of the least dose (loading dose 4 g over 30 minutes) to decrease the risk of side effects.
Conclusion. It is recommended to use MgSO4 for neuroprotection as it is a safe feasible effective and efficient method as well as it can prevent the trans cranial ultrasound positive findings for encephalopathy. MgSO4 prevents cerebral palsy by age 2, but its effect on cognition and behavior at school age remains uncertain and warrants further study.
REVIEW ARTICLES
What is already known about this subject?
► Venous thromboembolism (VTE) is the third lead cause of cardiovascular mortality with economic burden comparable to that of stroke, reaching tens of billions of dollars largely due to indirect costs.
► Post-thrombotic syndrome (PTS) develops in 20–50 % of deep vein thrombosis (DVT) patients, and chronic thromboembolic pulmonary hypertension (CTEPH) occurs in 0.5–4.0 % of pulmonary embolism (PE) survivors, both leading to permanent disability.
► Up to 39 % of patients suffer from psychological disorders post-VTE, and over half of physicians report a lack of multidisciplinary teams in their institutions to manage such patients.
What are the new findings?
► It substantiates the concept that VTE is a chronic disease requiring not just acute-phase treatment but rather a continuous "chronic disease management" process, including rehabilitation.
► It systematically details approaches to both subjective and objective methods for assessing quality of life and health outcomes in VTE patients.
► It summarizes comprehensive rehabilitation strategies for VTE patients, encompassing pharmacological support, physical interventions, psychosocial correction, and telemedicine technologies.
How might it impact on clinical practice in the foreseeable future?
► The implementation of the presented algorithms and multidisciplinary approach has a potential to markedly enhance effectiveness of rehabilitation and secondary prevention for VTE patients.
► The use of telemedicine and mobile apps for compliance monitoring will enable remote patient management, solving an issue of treatment adherence and the limited accessibility of rehabilitation services in remote regions.
► The development of predictive models based on artificial intelligence will allow for identification of high-risk groups for developing PTS and CTEPH, enabling early initiation of intensive rehabilitation interventions.
Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), remains a global health challenge. Modern advances in the management of acute VTE, such as the introduction of direct oral anticoagulants and interventional techniques, have led to a significantly decreased mortality rate, that however was simultaneously accounted for by a growing population of patients living with long-term disabling sequelae. The key complications are post-thrombotic syndrome (PTS) developing in 20–50 % of DVT patients that manifests as chronic venous insufficiency, edema, pain, and venous ulcers as well as chronic thromboembolic pulmonary hypertension (CTEPH), which occurs in up to 4.0 % of PE survivors and leads to progressive dyspnea, heart failure, and reduced exercise tolerance. The pathogenesis of these conditions is based on incomplete vein recanalization, valvular damage, persistent inflammation, and endothelial dysfunction in PTS, as well as thrombus organization and pulmonary vascular remodeling resulting in right heart failure in CTEPH. This article emphasizes the necessity to shift from an acute-event treatment model to a continuous chronic disease management paradigm. Effective rehabilitation requires a comprehensive multidisciplinary assessment, utilizing subjective scales and questionnaires alongside objective methods (duplex ultrasound, echocardiography, and cardiopulmonary exercise testing). Key components of a rehabilitation program include optimization of anticoagulation, nutritional support, compression therapy, early mobilization, and structured physical training to enhance the muscle-venous pump mechanism and cardiorespiratory fitness, as well as psychosocial support and lifestyle modification. VTE rehabilitation despite obvious demand faces a lack of standardized protocols, a scarcity of high-quality research, and unequal access to specialized care. Future directions include personalizing programs through risk stratification, utilizing telemedicine to improve treatment adherence, and developing clinical guidelines focused on long-term functional recovery and improved patients’ quality of life.
What is already known about this subject?
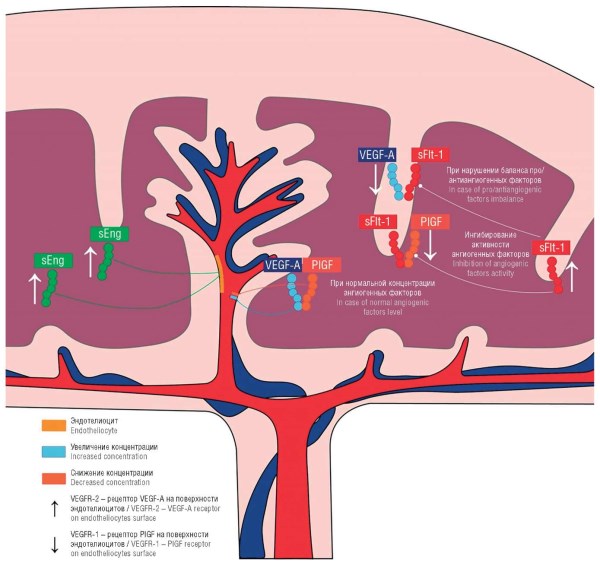
► An imbalance between pro- and anti-angiogenic factors – soluble fms-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PlGF) is one of the key pathogenetic mechanisms of preeclampsia (PE) and fetal growth restriction (FGR) in pregnant women.
► Dysfunctional placenta and endothelium along with oxidative stress underlies pregnancy complications.
► Metabolomics enables the detection of specific metabolic changes associated with pathological pregnancies.
What are the new findings?
► Disturbances in lipid (sphingomyelins, phospholipids) and amino acid (arginine, isoleucine) metabolism precede the imbalance in angiogenic factors and have a high diagnostic potential.
► Combined multi-marker panels incorporating angiogenic and metabolomic biomarkers demonstrate significantly higher diagnostic and prognostic accuracy compared to separate markers. For example, a metabolite panel (sphingomyelins SM C28:1, SM C30:1 and lysophospholipids LysoPC C19:0, LysoPE C20:0) in the second trimester shows superior predictive value compared with the sFlt-1/PlGF ratio in diagnosing РЕ, and the combined analysis of lysophosphatidylcholine C22:5 (LysoPC C22:5) and tryptophan in women with systemic lupus erythematosus, which yields high accuracy in predicting adverse pregnancy outcomes, comparable with assessing sFlt-1/PlGF.
How might it impact on clinical practice in the foreseeable future?
► The implementation of these technologies into routine clinical practice will enable early, preclinical diagnosis and risk stratification of pregnant women for pregnancy complications (PE, FGR, gestational diabetes mellitus).
► Metabolomic analysis opens avenues for developing personalized and targeted therapeutic strategies aimed at correcting metabolic disturbances.
► Understanding the interplay between the pathogenetic arms of angiogenesis and metabolism facilitates proposing updated algorithms for monitoring pregnancy progression and assessing response to therapy.
Introduction. A favorable pregnancy outcome is determined by normally functioning fetoplacental complex. Complications such as preeclampsia (РЕ) and fetal growth restriction (FGR) are associated with disturbed placental angiogenesis and systemic changes in maternal metabolism posing a risk of perinatal pathology.
Aim: to systematize data regarding a relationship between disorders of placental angiogenesis and alterations in the maternal metabolomic profile, substantiating their combined impact on developing pregnancy complications.
Results. An imbalanced angiogenic factors is a central pathogenetic mechanism that includes: increased soluble fms-like tyrosine kinase-1 (sFlt-1) and decreased placental growth factor (PlGF) level. This leads to endothelial dysfunction, oxidative stress, and systemic inflammation. Metabolomics analysis reveals specific shifts: in РЕ – disturbed phospholipid and amino acid metabolism (arginine, isoleucine); in FGR – altered amino acid and energy metabolism; in gestational diabetes mellitus – early changes in lipid profile and acylcarnitines. These metabolic disturbances often precede clinical manifestation. Combined multi-marker panels, incorporating angiogenic and metabolic biomarkers, demonstrate superior diagnostic and prognostic accuracy compared to individual markers.
Conclusion. Integrative assessment of angiogenic and metabolic markers lays a foundation for early preclinical diagnosis, risk stratification, and the development of targeted therapeutic strategies. Implementing multi-marker panels into clinical practice can markedly improve quality of pregnancy monitoring, prediction of pregnancy outcomes, and ensure timely intervention.
What is already known about this subject?
► Prevalence of endometrial polyps peak during the reproductive period being associated with about 35 % of infertility cases and 50 % of abnormal uterine bleeding.
► The recurrence rate following polypectomy varies from 14.2 to 45.5 %. Risk factors include the polyp histological type, high initial number of polyps, and follow-up duration.
► Currently, several theories regarding origin of endometrial polyps exist including altered endometrial tissue response to estrogen and progesterone, gene mutations, increased activity of signaling pathways inducing proliferation and angiogenesis; disrupted apoptosis are related to prolonged high-estrogen-level-stimulation and ongoing chronic inflammation in the endometrium.
What are the new findings?
► This review provides a comprehensive approach to analyzing various potential risk factors and pathogenetic mechanisms involved in the development and recurrence of endometrial polyps, thereby allowing to identify common signs they share.
► Aspects for further research aimed at revealing markers to predict development of endometrial polyp recurrence followed by identifying risk groups have been determined.
► Based on the pro-inflammatory hypothesis, it is emphasized to continue investigating markers of endometrial polyp recurrence in conjunction with uterine microbiome.
How might it impact on clinical practice in the foreseeable future?
► A comprehensive study of the endometrial microbiome and identifying factors contributing to the development of endometrial polyps may help to reveal predictors for polyp development, as well as related preventive and therapeutic methods.
► Knowledge of the pathogenetic mechanisms involved in emerging endometrial polyps may allow for developing effective methods for the treatment and prevention of this disease.
► This will allow to optimize management of patients with endometrial polyps, reducing the number of intrauterine interventions and increasing the likelihood of successful pregnancy.
Introduction. Endometrial polyposis is a common gynecological disease, resulting in benign overgrowths of endometrial tissue and being associated with abnormal uterine bleeding, infertility, and recurrent implantation failure. The recurrence rate following polypectomy varies from 14.2 to 45.5 %, leading to repeated intrauterine interventions and posing a significant obstacle to pregnancy achievement. Further research is needed to identify predictors of endometrial polyp recurrence and potential preventive strategies.
Aim: to study and analyze scientific data on endometrial polyps related to underlying pathogenesis, diagnosis, and prevention methods.
Materials and Methods. The literature search was conducted in the electronic databases eLibrary.ru, CyberLeninka, PubMed/ MEDLINE for the period 2015–2025 using keywords and phrases in Russian and English: «endometrial polyps», «pathogenesis», «endometrial polyps recurrence», «polypectomy», «chronic endometritis». Publications reporting original research findings were selected for analysis. The scientific data analysis included various inflammatory markers, their role in predicting endometrial polyp recurrence, and potential preventive measures.
Results. The current scientific concept considers endometrial polyps and chronic endometritis (CE) as stages of a single pathological process resulting from chronic inflammation as evidenced by similarities in dysregulated pathogenetic pathways and the uterine microbiome therein. It has been found that the majority of infertile patients with endometrial polyps show CE signs (51–92.6 %). CE markedly increases a risk of endometrial polyp recurrence post-resection. In addition, a risk of endometrial polyp recurrence correlates with CE severity. However, in most cases, hysteroscopic polypectomy alone was sufficient to treat CE with endometrial polyps without antibiotic therapy. Moreover, inappropriate antibiotic therapy may not only be ineffective but also delay recovery from CE, reduce the efficacy of CE-related polypectomy and increase the frequency of endometrial polyp recurrence. This suggests a need to identify predictors of endometrial polyp recurrence to determine risk groups and optimize management strategies for such patients. Analyzing scientific publications revealed significant differences in the levels of CD138 (plasma cell marker), CD20 (B-cell lymphocyte marker), CD8 (cytotoxic T-cell lymphocyte marker), matrix metalloproteinases, cyclooxygenase 2, and proteins of the Hippo-YAP1 and Wnt signaling pathways in endometrial polyp tissue compared to normal endometrium. Additionally, a decreased and altered uterine microbiota diversity were observed, which may be promising to seek out for markers predicting endometrial polyp recurrence.
Conclusion. The high prevalence and recurrence of endometrial polyps related to chronic endometritis, along with shared pathogenetic mechanisms, suggests that factors associated with CE could may serve as potential predictors of endometrial polyp recurrence. Comprehensively investigated uterine microbiome and factors contributing to endometrial polyp development build up a relevant and promising strategy promoting uncovering related to development of this pathology, optimizing management for patients with endometrial polyp recurrence as well as proposing pathogenesis-driven preventive and therapeutic approaches.
What is already known about this subject?
► Inositols are involved in regulating insulin, androgen (testosterone), and estrogen metabolism. D-chiroinositol (D-CI) is essential for functioning of signaling pathways underlying biological effects coupled to insulin receptors, reproductive hormones, and regulation of aromatase activity.
► Increased extragonadal aromatase expression along with hyperandrogenism in patients with polycystic ovary syndrome (PCOS) is reduced by using inositols – myoinositol (MI) and D-CI as insulin secondary messengers.
► Analyzing inositol stereoisomers revealed significant differences in the pharmacological effects mediated by MI and D-CI. A dose-dependent relationship was established between D-CI and aromatase (CYP19A1) activity in estrogen-dependent hyperproliferative disorders.
What are the new findings?
► Hormone-dependent proliferation is induced by special active estrogen metabolites 2-hydroxyestrone (2-OHE1) and 16α-hydroxyestrone (16α-OHE1), the ratio of which with testosterone regulates proliferative processes.
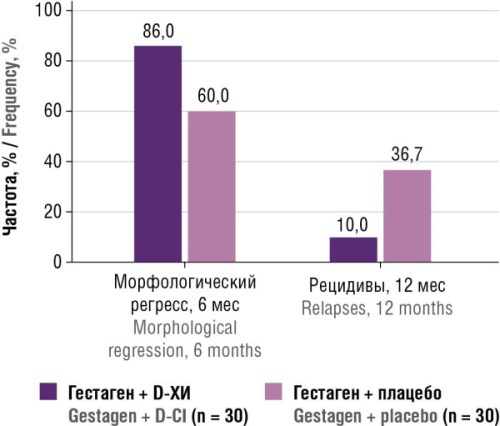
► D-CI effectively counteracts the pathophysiology of endometriosis, uterine fibroids, menstrual cycle disorders, and PCOS.
► Monotherapy with high dose D-CI and combination therapy with dienogest (DG) at lower doses significantly reduced the quantity, size and vascularization of endometriotic lesions compared to the control.
How might it impact on clinical practice in the foreseeable future?
► D-CI monotherapy significantly downregulates SIRT1 gene (sirtuin-1, a marker of aging) expression and increases the level of E-cadherin (a marker of slowed development of endometriosis as well as ectopic foci).
► Intake of D-CI reduced cell proliferation (assessed by histological marker PCNA) and developing small blood vessel network (assessed by marker CD34), as well as downregulated aromatase (CYP19A1) expression.
► In patients treated with D-CI and DG, regulation/normalization of the Ki-67 proliferation index (9.8 ± 4.5 %, normal: < 10 %) and VEGF expression (1.83 ± 0.53 units, normal: < 2.0 units) was observed. D-CI as part of combination therapy reduces the HOMA-IR index (2.44 ± 0.56 vs. 3.23 ± 0.52; p < 0.001), improves the lipid profile (decreased total cholesterol, low-density lipoproteins, triglycerides – by 1.2–1.4-fold; high-density lipoproteins increased by 1.3-fold).
D-chiroinositol (D-CI) is an endogenous molecule that plays a key role in the insulin signaling cascade. Insulin promotes the release of inositolphosphoglycans, which contain D-CI so that D-CI deficiency in cells and tissues is directly related to insulin resistance. The mechanism of action of all insulin sensitizers is linked to increasing free D-CI concentration. However, the role of D-CI in vivo is not limited to mediating insulin signal transduction, as it is also involved in the dose-dependent regulation of various other essential physiological processes. This enables D-CI-level-based modulation of distinct physiological functions. D-CI dose-dependently modulates the activity of key steroidogenic enzymes, including 17α-hydroxylase, 3β-hydroxysteroid dehydrogenase, and aromatase. It also exhibits anti-inflammatory and anti-tumor properties by downmodulating levels of tumor necrosis factor-alpha (TNF-α) and nuclear factor kappa B (NF-κB), as well as suppressing integrin β3 (protein that in humans is encoded by the ITGB3 gene) gene expression. These effects underpin potential D-CI therapeutic efficacy in managing a broad spectrum of reproductive system disorders. D-CI-related multifaceted effects on insulin resistance, steroidogenesis regulation, and inflammation position this molecule as a promising pharmaconutrient for correcting a wide range of conditions – spanning from insulin resistance syndrome with hyperandrogenism in polycystic ovary syndrome to hyperproliferative, estrogen-dependent diseases such as endometriosis, uterine fibroids, endometrial hyperplasia, and fibrocystic breast disease. The selection of appropriate D-CI daily dosage is a critical determinant underlying its full clinical efficacy.
What is already known about this subject?
► Cervical cancer (СС) frequently affects women of reproductive age, necessitating development of fertility-preserving approaches.
► Radical trachelectomy is the standard for fertility preservation in early-stage СС in selected patients.
► Fertility-sparing surgeries show oncological outcomes comparable to radical treatment while preserving fertility.
What are the new findings?
► Modern fertility preservation strategies at various СС stages are systematized, including pre-surgery neoadjuvant chemotherapy for tumor size reduction.
► The effectiveness of less radical interventions (simple trachelectomy, conization) with a high pregnancy rate has been analyzed.
► Key success factors are identified as follows: tumor size ≤ 2 cm, no lymphovascular space invasion, and careful patient selection.
How might it impact on clinical practice in the foreseeable future?
► Expanded indications for fertility-sparing СС treatment through neoadjuvant chemotherapy.
► Implementing personalized approach to selection method based on tumor characteristics and reproductive plans.
► Development of multidisciplinary collaboration between gynecologic oncologists and reproductive specialists to improve outcomes.
Introduction. Cervical cancer (CC) is a leading cause of reproductive function loss and the most common oncological pathology of the female reproductive system. Modern treatment methods (surgical, radiation, chemotherapeutic) increase survival but often result in infertility. Therefore, the development of organ-preserving approaches that allow fertility preservation is relevant.
Aim: to analyze available publications assessing preservation of reproductive function after СС treatment, effectiveness of methods, and identify key success factors.
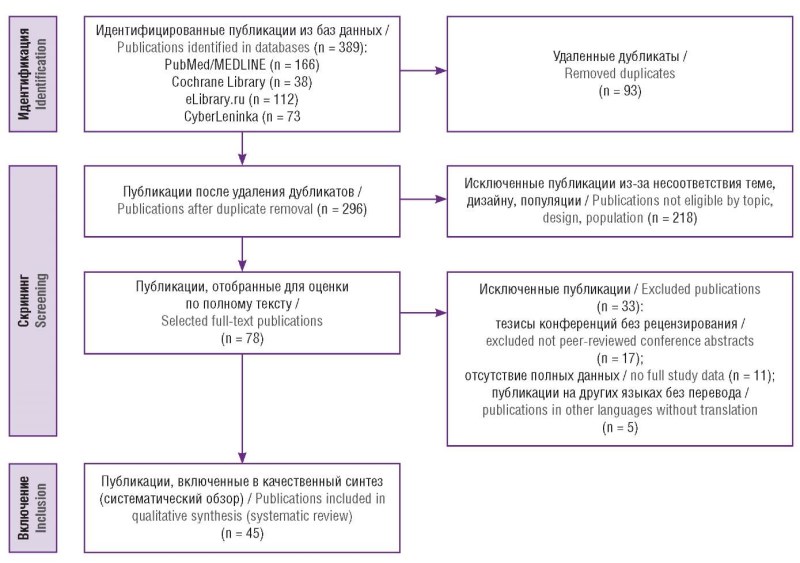
Materials and Methods. A systematic review was conducted in accordance with the PRISMA 2020 guidelines. The search for publications from 2000 to 2025 was performed in PubMed/MEDLINE, Cochrane Library, eLibrary.ru, and CyberLeninka databases. The selection process identified 45 publications that met the inclusion criteria: original research, systematic reviews, meta-analyses, and clinical cases describing fertility-sparing strategies providing data on oncological and reproductive outcomes.
Results. Modern organ-preserving methods, including various types of trachelectomy, conization, neoadjuvant chemotherapy, and assisted reproductive technologies, allow achieving oncological safety while preserving reproductive potential in selected patients with early-stage СС.
Conclusion. Modern organ-preserving approaches in СС treatment hold a promise in oncogynecology, enabling the combination of treatment radicality with the maintenance of reproductive capabilities.
What is already known about this subject?
► Preeclampsia (PE) is a serious pregnancy complication rooted in placental dysfunction and systemic inflammation.
► Physiological pregnancy is characterized by the expansion of paternal antigen-specific regulatory T cells (Tregs), which maintain immune homeostasis at the maternal-fetal interface.
► The complement system, a key arm of innate immunity, is activated in various pathological processes.
What are the new findings?
► In PE, Tregs quantitative and functional deficit is observed, lea-
ding to imbalanced level of these cells skewed towards type 17 T-helper subset (Th17) and systemic inflammation.
► There is hyperactivation of the complement system, evidenced by elevated levels of C3a, C5a, and the membrane attack complex (C5b-9), which directly damages the trophoblast and endothelium.
► A critical finding is the bidirectional crosstalk between Tregs and the complement system: C3a and C5a receptors (C3aR/C5aR) activation suppresses Treg function, whereas Treg deficiency weakens control over complement activation. A vicious cycle of immune dysregulation is established, underpinning defective placentation and PE clinical manifestation.
How might it impact on clinical practice in the foreseeable future?
► New targeted strategies aimed at restoring Treg balance and suppressing pathological complement activity are now being developed.
► Insights into the immune mechanisms may contribute to developing new biomarkers for PE early diagnosis and risk assessment.
► Immunomodulatory therapy targeting this vicious cycle could become a novel approach for PE prevention.
Preeclampsia (PE) is a pregnancy complication characterized by arterial hypertension, proteinuria, and multi-organ dysfunction. This review is dedicated to analyzing data on the role of immune system dysregulation in PE pathogenesis, by focusing on two key components: impaired regulatory T cells (Treg) function and hyperactivation of the complement system. Under normal conditions, pregnancy involves the establishment of immune tolerance to the semi-allogeneic fetus, a central element of which is presented by a pool of paternal antigen-specific Tregs. In PE, a Treg quantitative and functional deficiency is observed, leading to an imbalance and a shift towards the proliferation of pro-inflammatory Th17 cells (T-helper 17 cells), which in turn causes systemic inflammation. Concurrently, there is an excessive activation of the complement system, evidenced by elevated anaphylatoxins level (C3a, C5a) and the formation of the membrane attack complex (C5b-9) in the blood and placental tissue. These components damage the trophoblast and endothelium, exacerbating placental dysfunction. A critical insight is the existence of a bidirectional crosstalk between these systems. The activation of anaphylatoxin receptors of complement components C3a and C5a (anaphylatoxin receptors C3a, C5a, C3aR/C5aR) destabilizes Tregs and interferes with their suppressive function, while the Treg deficiency, in turn, weakens the control over complement activation processes, partly due to reduced production of anti-inflammatory cytokines – interleukin-10 (IL-10), transforming growth factor-beta (TGF-β). This self-perpetuating cycle of immune dysregulation underlies the impairment of placentation, systemic endothelial dysfunction, and PE clinical manifestation. Understanding these interconnected mechanisms opens prospects for developing novel targeted strategies aimed at restoring the Treg balance and suppressing pathological complement activity to prevent PE.
CLINICAL CASE
What is already known about this subject?
► Hyperthyroidism affects approximately 0.05 % of women of reproductive age, most commonly due to Graves’ disease.
► Physiological tachycardia is common during pregnancy and may mask underlying pathological conditions.
► Delayed detection and treatment of maternal hyperthyroidism significantly increase the risk of adverse maternal and fetal outcomes.
What are the new findings?
► Tachycardia during early pregnancy should not be solely attributed to common complications like hyperemesis gravidarum; hyperthyroidism must also be considered.
► A poor response to initial treatment for dehydration warrants a broader differential diagnosis beyond hypovolemia, specifically including Graves’ disease.
► Rapid diagnosis via TSH and fT4 evaluations enables prompt treatment and promotes favorable clinical outcomes.
How might it impact on clinical practice in the foreseeable future?
► It strongly encourages early thyroid function screening in pregnant women who present with unexplained tachycardia.
► This clinical case raises clinical awareness that tachycardia may indicate hyperthyroidism, even in the absence of classic symptoms such as goiter or ophthalmopathy.
Introduction. Hyperthyroidism occurs in 35–50 per 100,000 women aged 20–29 years annually. Pregnancy outcomes in hyperthyroid mothers depend heavily on metabolic control. This case report discusses a pregnant patient with Graves' disease who presented without the typical symptoms of hyperthyroidism or thyrotoxicosis.
Case report. A 31-year-old multiparous woman (gravida 3, para 2) at 38 weeks of gestation was admitted to a tertiary care center in labor. She had previously visited the emergency room due to severe diarrhea, dehydration, and hyperthyroidism. The patient received regular antenatal care at an endocrine clinic, where she was treated with propylthiouracil and propranolol until her seventh month of pregnancy. Subsequent evaluations revealed normalized thyroxine (T4) and thyroid-stimulating hormone (TSH) levels; thus, the treatment was concluded. The patient underwent an uncomplicated vaginal delivery and was safely discharged.
Discussion. The patient had no prior history of thyroid disorders. Her initial symptoms emerged at two months of gestation, presenting as vomiting, dehydration, tachycardia, and weight loss. While an initial diagnosis of dehydration seemed to explain the tachycardia, laboratory tests revealed low TSH and increased free T4 (fT4) levels, confirming hyperthyroidism despite the absence of classic physical signs. Implementing maternal thyroid disorder screening to prevent such complications align with similar initiatives in Indonesia, such as the Congenital Hypothyroidism Screening program. However, expert guidelines from the American Thyroid Association and the Endocrine Society do not currently recommend universal thyroid screening in the absence of specific risk factors.
Conclusion. Optimal pregnancy outcomes in hyperthyroid patients require early diagnosis and adequate treatment. Tachycardia presenting during early pregnancy should be investigated for underlying causes other than dehydration. Although universal thyroid screening in early pregnancy is not recommended without risk factors, strong clinical suspicion remains a clear indication for further laboratory examination.
FROM HISTORY
Introducing obstetric anesthesia in the 19th century marked a pivotal stage in the development of medicine, fundamentally transforming the understanding that pain plays in childbirth. The work by James Young Simpson led to the widespread use of chloroform for labor analgesia and demonstrated an opportunity for safe and effective pain control. Simpson’s contributions were of the paramount importance for humanization of obstetric care and emergence of anesthesiology as an independent medical discipline, thereby highlighting a transition from the acceptance of pain to its targeted management.
EVENTS

Events
2026-03-23
Take a survey for healthcare professionals on the use of artificial intelligence in healthcare
Survey: The use of AI technologies in medical activities
Direct hyperlink: https://anketolog.ru/rs/1013120/Ea6s6qUk
QR-code:

| More Events... |

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
ISSN 2500-3194 (Online)






































